

Neoadjuvant treatment for locally advanced unresectable and borderline resectable pancreatic cancer: oncological outcomes at a single academic centre
- PMID: 33229503
- PMCID: PMC7684818
- DOI: 10.1136/esmoopen-2020-000929
Neoadjuvant treatment for locally advanced unresectable and borderline resectable pancreatic cancer: oncological outcomes at a single academic centre
Abstract
Introduction: Pancreatic cancer (PC), even in the absence of metastatic disease, has a dismal prognosis. One-third of them are borderline resectable (BRPC) or locally advanced unresectable PC (LAUPC) at diagnosis. There are limited prospective data supporting the best approach on these tumours. Neoadjuvant chemotherapy (ChT) is being increasingly used in this setting.
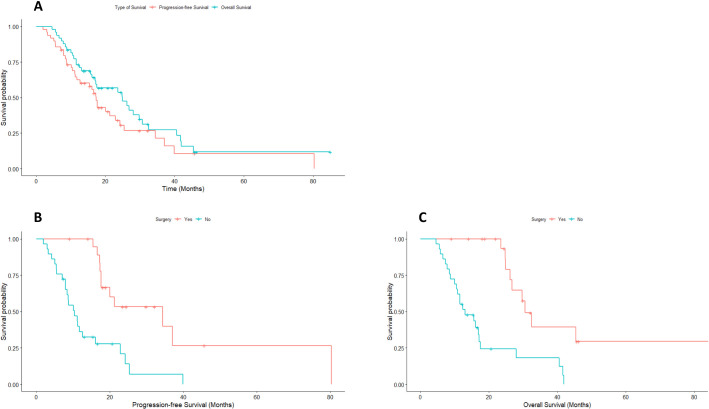
Methods: This is a retrospective series of consecutive patients staged as BRPC or LAUPC after discussion in the multidisciplinary board (MDB) at an academic centre. All received neoadjuvant ChT, followed by chemoradiation (ChRT) in some cases, and those achieving enough downstaging had a curative-intent surgery. Descriptive data about patient's characteristics, neoadjuvant treatments, toxicities, curative resections, postoperative complications, pathology reports and adjuvant treatment were collected. Overall survival (OS) and progression-free survival was calculated with Kaplan-Meier method and log-rank test.
Results: Between August 2011 and July 2019, 49 patients fulfilled the inclusion criteria, and all of them received neoadjuvant ChT. Fluorouracil+folinic acid, irinotecan and oxaliplatin was the most frequently used scheme (77%). The most prevalent grade 3 or 4 toxicities were neutropenia (26.5%), neurotoxicity (12.2%), diarrhoea (8.2%) and nausea (8.2%). 18 patients (36.7%) received ChRT thereafter. In total, 22 patients (44,9%) became potentially resectable and 19 of them had an R0 or R1 pancreatic resection. One was found to be unresectable at surgery and two refused surgery. A vascular resection was required in 7 (35%). No postoperative deaths were observed. Postoperative ChT was given to 12 (66.7%) of resected patients. Median OS of the whole cohort was 24,9 months (95% CI 14.1 to 35.7), with 30.6 months for resected and 13.1 months for non-resected patients, respectively (p<0.001).
Conclusion: A neoadjuvant approach in BRPC and LAUPC was well tolerated and allowed a curative resection in 38.8% of them with a potential improvement on OS.
Keywords: FOLFIRINOX; borderline resectable; locally advanced unresectable; neoadjuvant therapy; pancreatic cancer.
© Author (s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. Published by BMJ on behalf of the European Society for Medical Oncology.
Conflict of interest statement
Competing interests: AC declares institutional research funding from Genentech, Merck Serono, BMS, MSD, Roche,Beigene, Bayer, Servier, Lilly, Novartis, Takeda, Astellas, Natera and Fibrogen and advisory board orspeaker fees from Merck Serono, Roche, Servier, Takeda, Natera and Astellas in the last 5 years. All remaining authors have declared no conflict of interest. LS has participated in the development of teaching resources, advisory and educational programs for Abbott, Mylan, Johnson and Johnson, Medtronic, Baxter and Prim.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
