

Ultrarare heterozygous pathogenic variants of genes causing dominant forms of early-onset deafness underlie severe presbycusis
- PMID: 33229591
- PMCID: PMC7733833
- DOI: 10.1073/pnas.2010782117
Ultrarare heterozygous pathogenic variants of genes causing dominant forms of early-onset deafness underlie severe presbycusis
Abstract
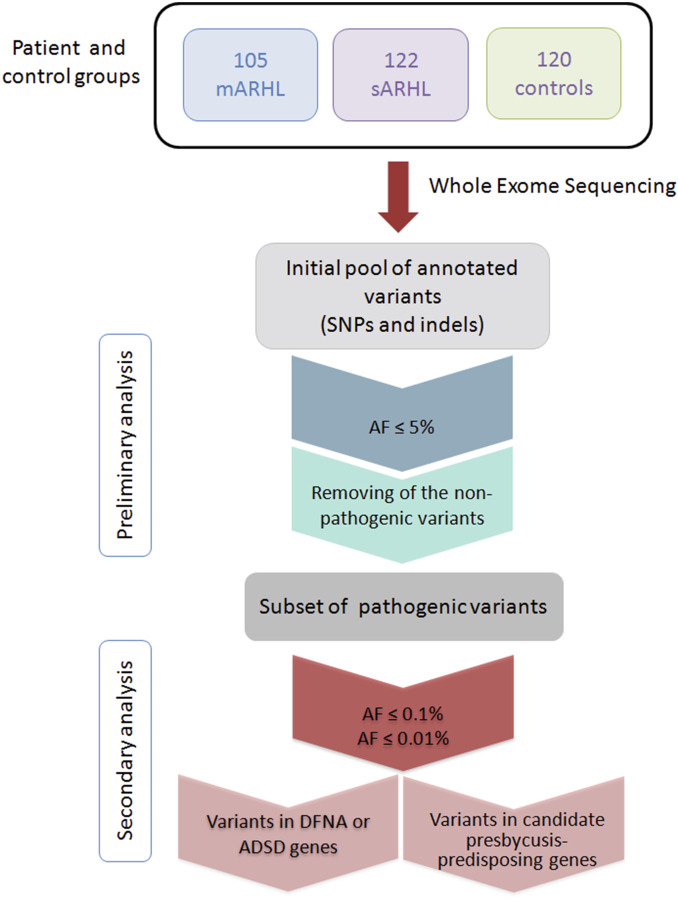
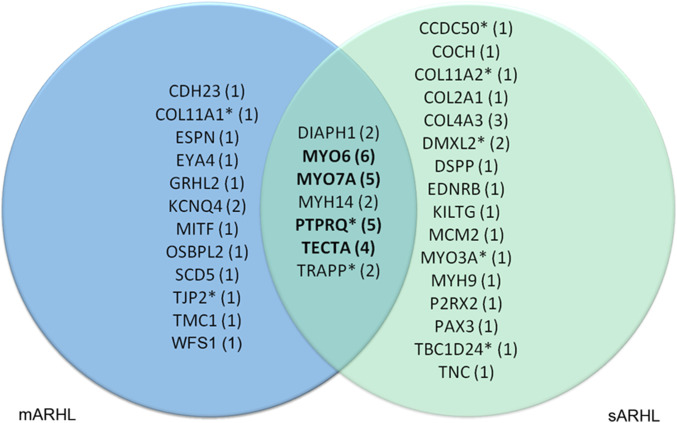
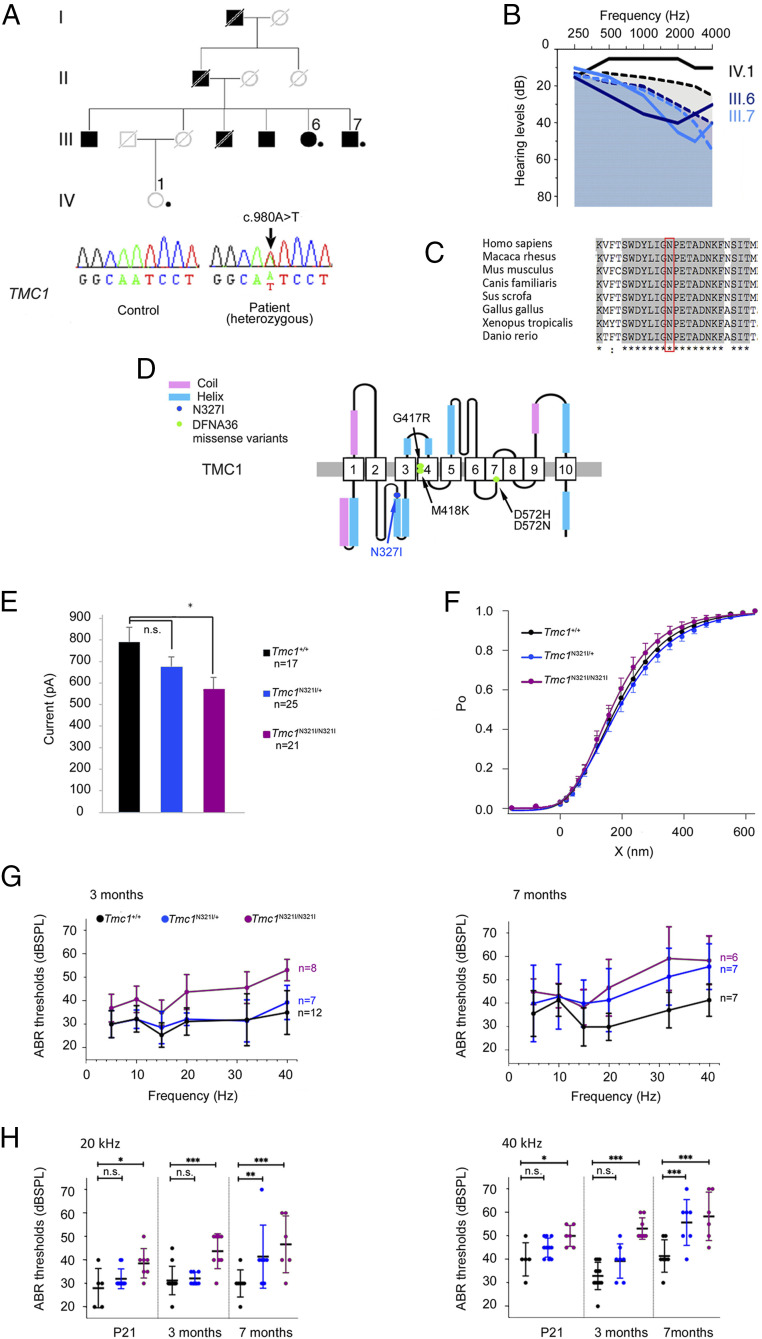
Presbycusis, or age-related hearing loss (ARHL), is a major public health issue. About half the phenotypic variance has been attributed to genetic factors. Here, we assessed the contribution to presbycusis of ultrarare pathogenic variants, considered indicative of Mendelian forms. We focused on severe presbycusis without environmental or comorbidity risk factors and studied multiplex family age-related hearing loss (mARHL) and simplex/sporadic age-related hearing loss (sARHL) cases and controls with normal hearing by whole-exome sequencing. Ultrarare variants (allele frequency [AF] < 0.0001) of 35 genes responsible for autosomal dominant early-onset forms of deafness, predicted to be pathogenic, were detected in 25.7% of mARHL and 22.7% of sARHL cases vs. 7.5% of controls (P = 0.001); half were previously unknown (AF < 0.000002). MYO6, MYO7A, PTPRQ, and TECTA variants were present in 8.9% of ARHL cases but less than 1% of controls. Evidence for a causal role of variants in presbycusis was provided by pathogenicity prediction programs, documented haploinsufficiency, three-dimensional structure/function analyses, cell biology experiments, and reported early effects. We also established Tmc1N321I/+ mice, carrying the TMC1:p.(Asn327Ile) variant detected in an mARHL case, as a mouse model for a monogenic form of presbycusis. Deafness gene variants can thus result in a continuum of auditory phenotypes. Our findings demonstrate that the genetics of presbycusis is shaped by not only well-studied polygenic risk factors of small effect size revealed by common variants but also, ultrarare variants likely resulting in monogenic forms, thereby paving the way for treatment with emerging inner ear gene therapy.
Keywords: Tmc1; age-related hearing loss; monogenic disorder; presbycusis; ultrarare variants.
Conflict of interest statement
The authors declare no competing interest.
Figures
References
-
- World Health Organization , Addressing the rising prevalence of hearing loss (2018). https://apps.who.int/iris/handle/10665/260336. Accessed 13 November 2020.
-
- Gates G. A., Mills J. H., Presbycusis. Lancet 366, 1111–1120 (2005). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
