

Surgical intervention combined with weight-bearing walking training improves neurological recoveries in 320 patients with clinically complete spinal cord injury: a prospective self-controlled study
- PMID: 33229715
- PMCID: PMC8178778
- DOI: 10.4103/1673-5374.297080
Surgical intervention combined with weight-bearing walking training improves neurological recoveries in 320 patients with clinically complete spinal cord injury: a prospective self-controlled study
Abstract
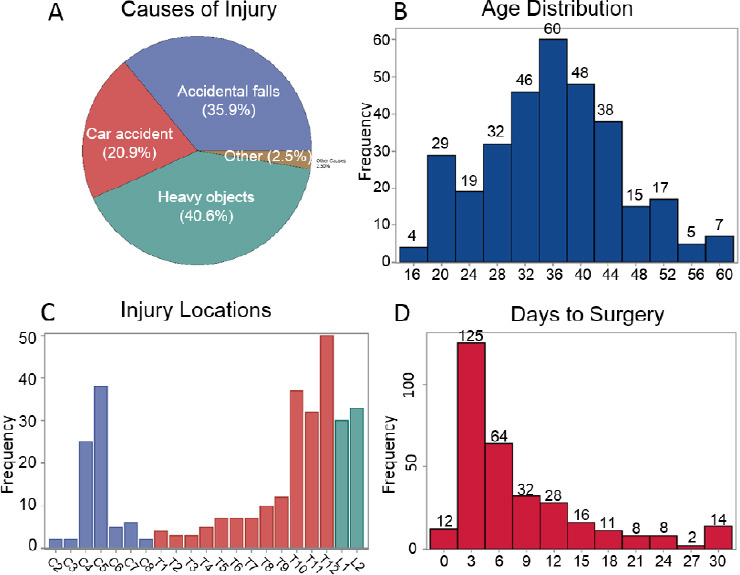
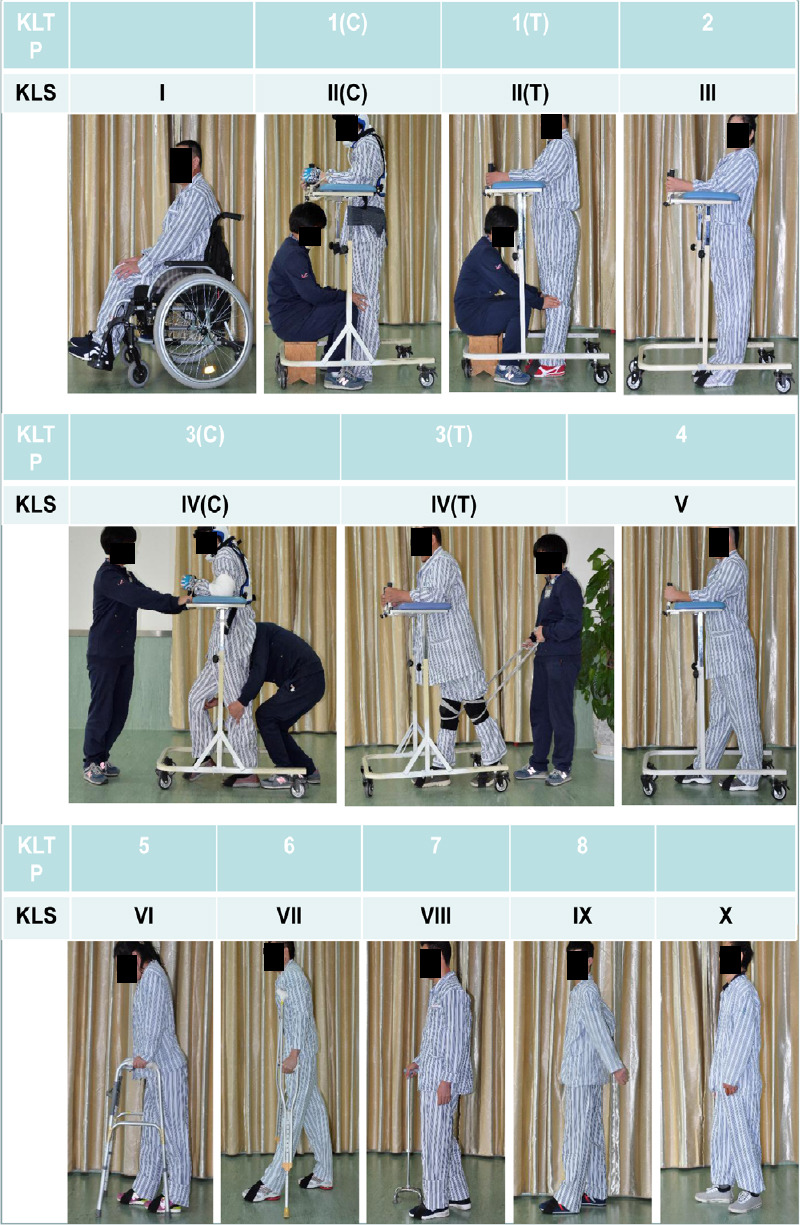
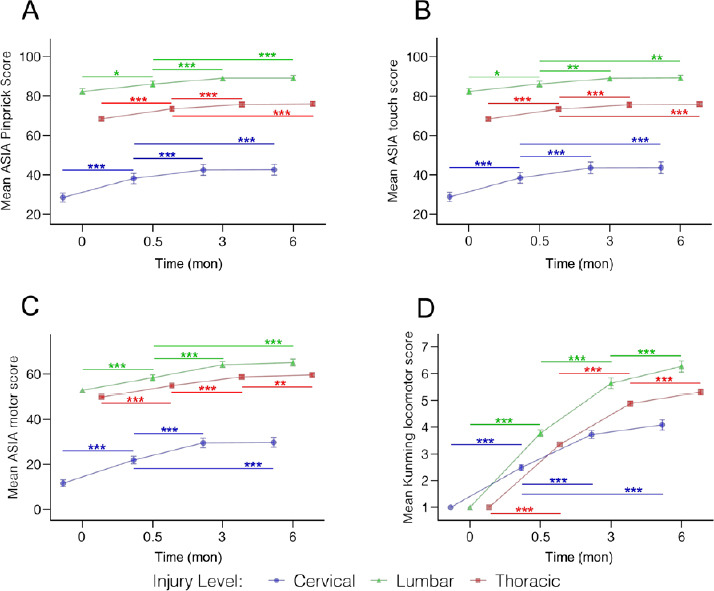
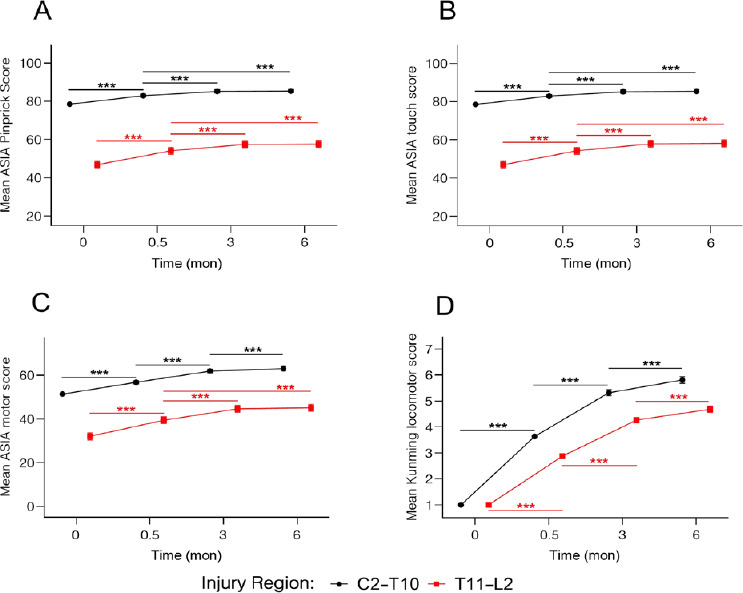
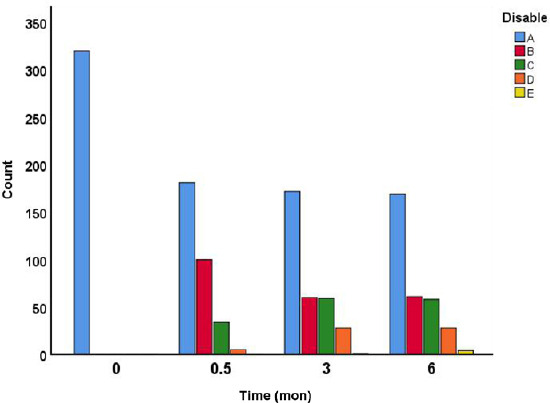
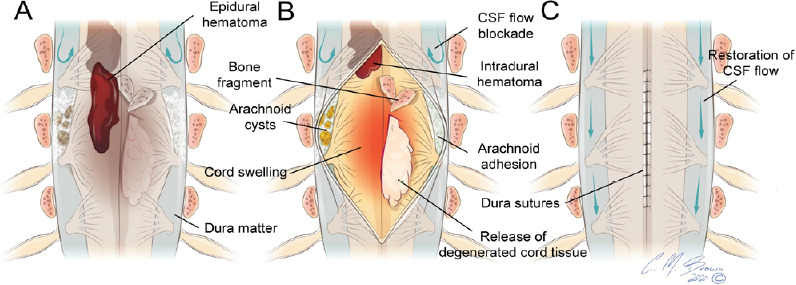
Although a large number of trials in the SCI field have been conducted, few proven gains have been realized for patients. In the present study, we determined the efficacy of a novel combination treatment involving surgical intervention and long-term weight-bearing walking training in spinal cord injury (SCI) subjects clinically diagnosed as complete or American Spinal Injury Association Impairment Scale (AIS) Class A (AIS-A). A total of 320 clinically complete SCI subjects (271 male and 49 female), aged 16-60 years, received early (≤ 7 days, n = 201) or delayed (8-30 days, n = 119) surgical interventions to reduce intraspinal or intramedullary pressure. Fifteen days post-surgery, all subjects received a weight-bearing walking training with the "Kunming Locomotion Training Program (KLTP)" for a duration of 6 months. The neurological deficit and recovery were assessed using the AIS scale and a 10-point Kunming Locomotor Scale (KLS). We found that surgical intervention significantly improved AIS scores measured at 15 days post-surgery as compared to the pre-surgery baseline scores. Significant improvement of AIS scores was detected at 3 and 6 months and the KLS further showed significant improvements between all pair-wise comparisons of time points of 15 days, 3 or 6 months indicating continued improvement in walking scores during the 6-month period. In conclusion, combining surgical intervention within 1 month post-injury and weight-bearing locomotor training promoted continued and statistically significant neurological recoveries in subjects with clinically complete SCI, which generally shows little clinical recovery within the first year after injury and most are permanently disabled. This study was approved by the Science and Research Committee of Kunming General Hospital of PLA and Kunming Tongren Hospital, China and registered at ClinicalTrials.gov (Identifier: NCT04034108) on July 26, 2019.
Keywords: American Spinal Injury Association Impairment Scale–A; functional recovery; human; intramedullary decompression; spinal cord injury; surgical intervention; walking training.
Conflict of interest statement
None
Figures

References
-
- Ahuja CS, Wilson JR, Nori S, Kotter MRN, Druschel C, Curt A, Fehlings MG. Traumatic spinal cord injury. Nat Rev Dis Primers. 2017a;3:17018. - PubMed
-
- Ahuja CS, Nori S, Tetreault L, Wilson J, Kwon B, Harrop J, Choi D, Fehlings MG. Traumatic spinal cord injury-repair and regeneration. Neurosurgery. 2017b;80:S9–22. - PubMed
-
- Anderberg L, Aldskogius H, Holtz A. Spinal cord injury--scientific challenges for the unknown future. Ups J Med Sci. 2007;112:259–288. - PubMed
-
- Anderson KD. Targeting recovery: priorities of the spinal cord-injured population. J Neurotrauma. 2004;21:1371–1383. - PubMed
-
- Belanger M, Drew T, Provencher J, Rossignol S. A comparison of treadmill locomotion in adult cats before and after spinal transection. J Neurophysiol. 1996;76:471–491. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
