

Intraductal Papillary Mucinous Neoplasm with Pancreatogastric Fistula
- PMID: 33229807
- PMCID: PMC8112989
- DOI: 10.2169/internalmedicine.5889-20
Intraductal Papillary Mucinous Neoplasm with Pancreatogastric Fistula
Abstract
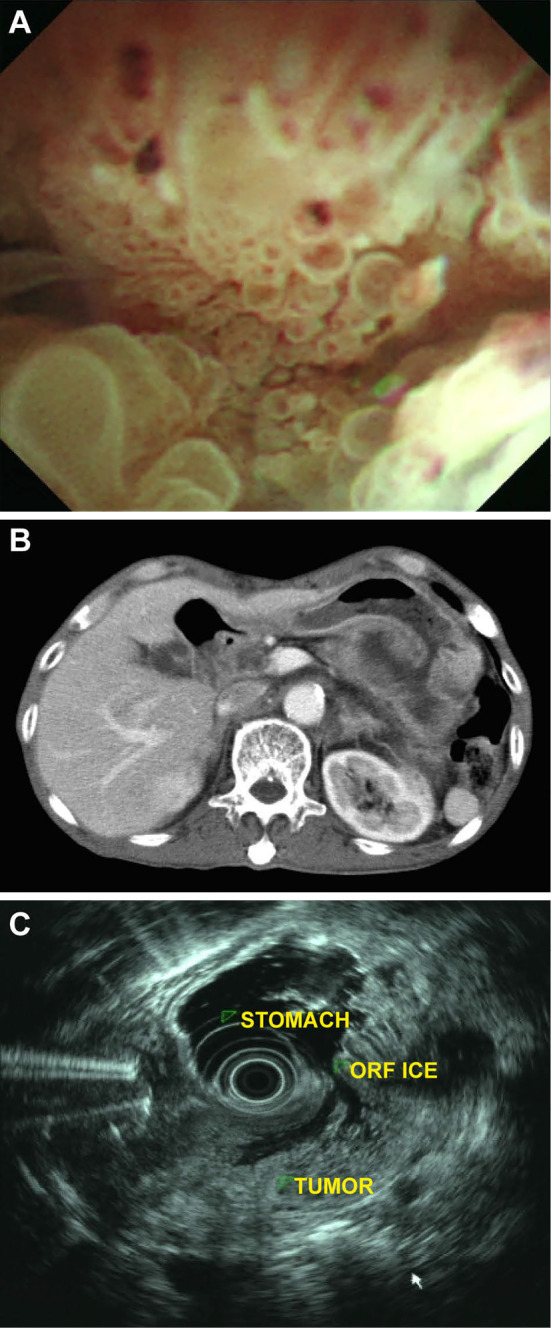
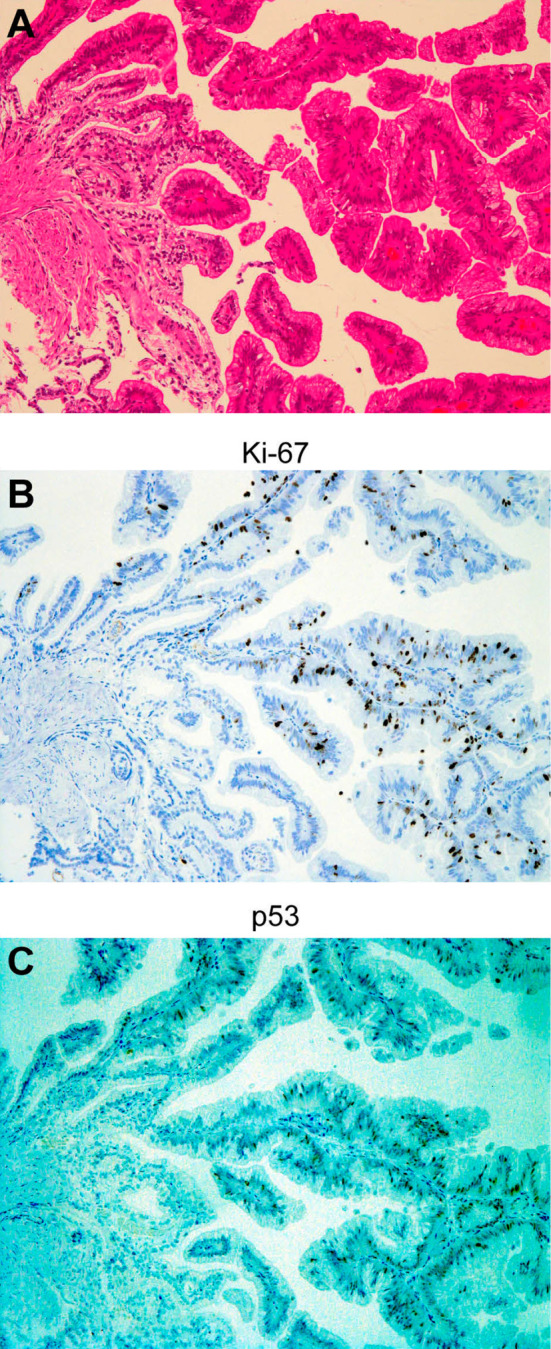
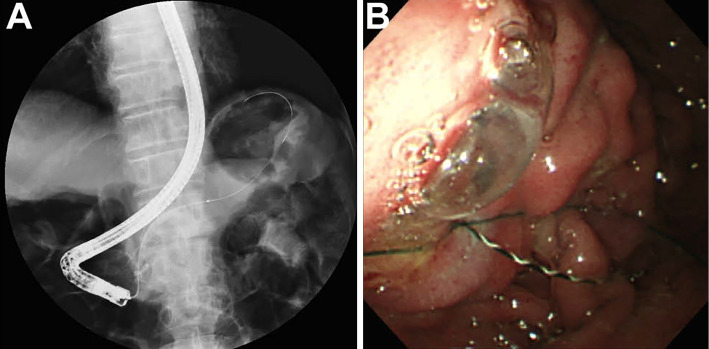
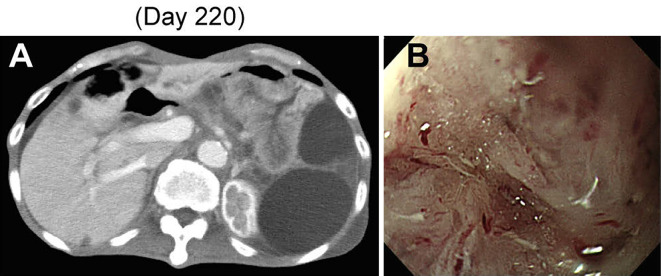
We herein report a rare case of intraductal papillary mucinous neoplasm with a pancreatogastric fistula in an elderly Japanese man admitted to our hospital. The pancreatogastric fistula was confirmed using endoscopic retrograde pancreatography via a cannulated guidewire placed in the stomach. Six months after admission, the patient was diagnosed with intraductal papillary mucinous carcinoma. A pancreatogastric fistula is generally a rare complication of intraductal papillary mucinous neoplasm. It was caused by mechanical penetration in this case. Interestingly, we also observed endoscopic and histochemical mucosal changes in the fistula.
Keywords: endoscopic retrograde cholangiopancreatography; intraductal papillary mucinous carcinoma; intraductal papillary mucinous neoplasm; mechanical penetration; pancreatogastric fistula.
Conflict of interest statement
Figures
Similar articles
-
Malignant intraductal papillary mucinous neoplasm of the pancreas with multiple pancreatogastric fistulas: a report of 2 cases with different features.Gastrointest Endosc. 2007 Oct;66(4):854-7. doi: 10.1016/j.gie.2007.01.019. Epub 2007 Aug 24. Gastrointest Endosc. 2007. PMID: 17719044 No abstract available.
-
Intraductal papillary-mucinous neoplasm of the pancreas penetrating to the stomach and the common bile duct.JOP. 2012 Jan 10;13(1):61-5. JOP. 2012. PMID: 22233949
-
A case of pancreaticobiliary fistula associated with an intraductal papillary mucinous neoplasm of the pancreas.Jpn J Clin Oncol. 2015 Feb;45(2):232. doi: 10.1093/jjco/hyu217. Jpn J Clin Oncol. 2015. PMID: 25589455 No abstract available.
-
Biliopancreatic fistula associated with intraductal papillary-mucinous pancreatic cancer: institutional experience and review of the literature.Hepatogastroenterology. 2000 Jul-Aug;47(34):1164-7. Hepatogastroenterology. 2000. PMID: 11020905 Review.
-
Hepatobiliary and Pancreatic: Intraductal papillary mucinous neoplasm rupture: A rare cause of pancreatic fistula.J Gastroenterol Hepatol. 2020 Apr;35(4):528. doi: 10.1111/jgh.14882. Epub 2019 Dec 10. J Gastroenterol Hepatol. 2020. PMID: 31822035 Review. No abstract available.
Cited by
-
Pancreatico-gastric fistula arising from IPMN associated with ductal adenocarcinoma of the pancreas: a case report and a literature review.Front Surg. 2023 May 24;10:1171234. doi: 10.3389/fsurg.2023.1171234. eCollection 2023. Front Surg. 2023. PMID: 37292487 Free PMC article.
References
-
- Ohashi K, Murakami Y, Maruyama M, et al. . Four cases of mucus-secreting pancreatic cancer (in Japanese). Prog Digest Endosc 20: 348-351, 1982.
-
- Tanaka M, Chari S, Adsay V, et al.; International Association of Pancreatology. International consensus guidelines for management of intraductal papillary mucinous neoplasms and mucinous cystic neoplasms of the pancreas. Pancreatology 6: 17-32, 2006. - PubMed
-
- Tanaka M, Fernández-del Castillo C, Adsay V, et al.; International Association of Pancreatology. International consensus guidelines 2012 for the management of IPMN and MCN of the pancreas. Pancreatology 12: 183-197, 2012. - PubMed
-
- Tanaka M, Fernandez-del Castillo C, Kamisawa T, et al.; International Association of Pancreatology. Revisions of international consensus Fukuoka guidelines for the management of IPMN of the pancreas. Pancreatology 6: 738-753, 2017. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical