

Reduction in movement-evoked pain and fatigue during initial 30-minute transcutaneous electrical nerve stimulation treatment predicts transcutaneous electrical nerve stimulation responders in women with fibromyalgia
- PMID: 33230010
- PMCID: PMC8049882
- DOI: 10.1097/j.pain.0000000000002144
Reduction in movement-evoked pain and fatigue during initial 30-minute transcutaneous electrical nerve stimulation treatment predicts transcutaneous electrical nerve stimulation responders in women with fibromyalgia
Abstract
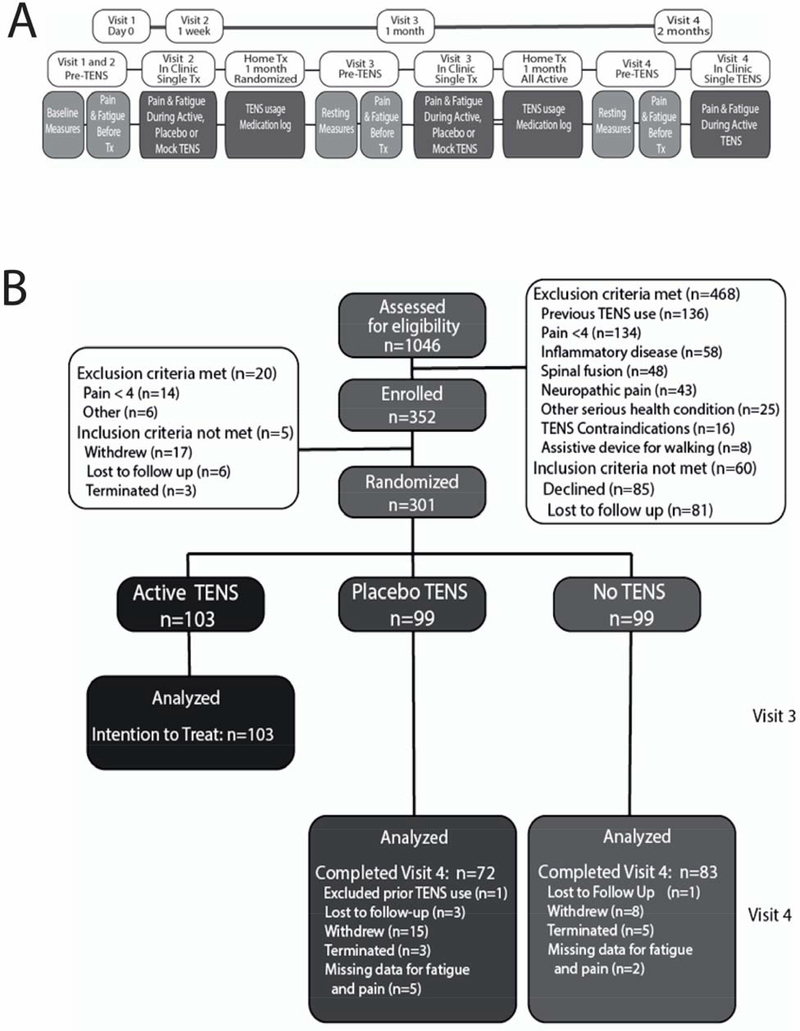
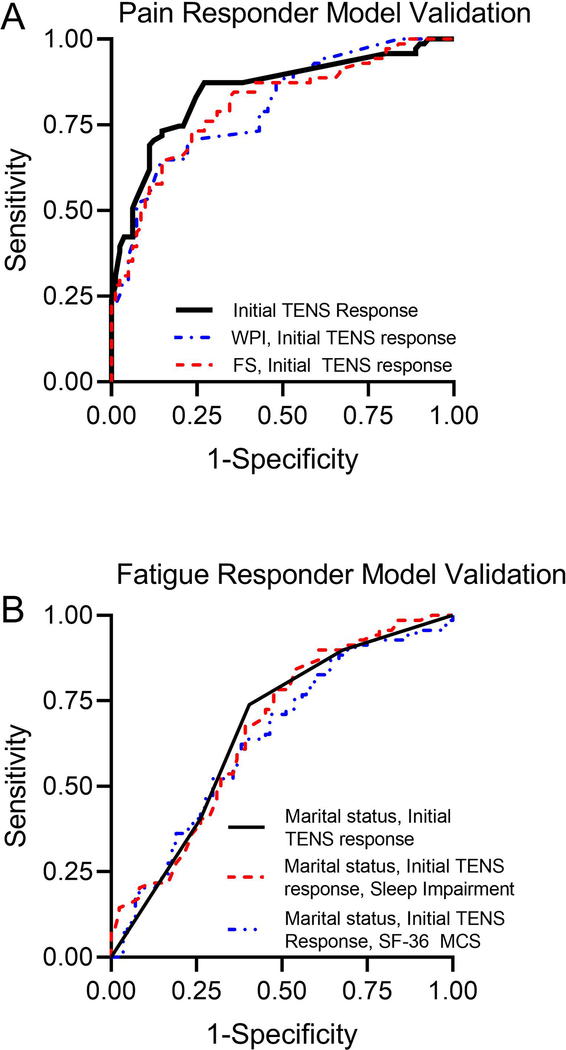
We previously showed that 1 month of transcutaneous electrical nerve stimulation (TENS) reduces movement-evoked pain and fatigue in women with fibromyalgia (FM). Using data from this study (Fibromyalgia Activity Study with TENS [FAST]), we performed a responder analysis to identify predictors of clinical improvement in pain and fatigue with TENS, validated these models using receiver operator characteristic, and determined number needed to treat and number needed to harm. Participants were randomly assigned to active-TENS (2-125 Hz; highest-tolerable intensity), placebo-TENS, or no-TENS for 1 month. At the end of the randomized phase, placebo-TENS and no-TENS groups received active-TENS for 1 month. The predictor model was developed using data from the randomized phase for the active-TENS group (n = 103) and validated using data from placebo-TENS and no-TENS groups after active-TENS for 1 month (n = 155). Participant characteristics, initial response to TENS for pain and fatigue, sleep, psychological factors, and function were screened for association with changes in pain or fatigue using a logistic regression model. Predictors of clinical improvement in pain were initial response to pain and widespread pain index (area under the curve was 0.80; 95% confidence interval: 0.73-0.87). Predictors of clinical improvement in fatigue were marital status, sleep impairment, and initial response to TENS (area under the curve was 0.67; 95% confidence interval: 0.58-0.75). Number needed to treat for pain and fatigue ranged between 3.3 and 5.3. Number needed to harm ranged from 20 to 100 for minor TENS-related adverse events. The response to an initial 30-minute TENS treatment predicts who responds to longer-term TENS use in women with FM, making this a clinically useful procedure. Number needed to treat and number needed to harm suggest that TENS is effective and safe for managing pain and fatigue in FM.
Trial registration: ClinicalTrials.gov NCT01888640.
Copyright © 2020 International Association for the Study of Pain.
Conflict of interest statement
Conflicts of Interest/Disclosure statement:
Kathleen A. Sluka, PT, PhD, FAPTA serves as a consultant for Novartis Consumer Healthcare/GSK Consumer Healthcare and Regeneron, Inc. Dr. Sluka receives royalties from IASP Press. The remaining authors of this manuscript have no conflicts of interest that compromise the integrity of this work.
Figures
References
-
- Allison PD. Logistic Regression Using SAS: Theory and Application, 2nd Ed. Cary, NC: SAS Institute Inc., 2012.
-
- Belza BL. Comparison of self-reported fatigue in rheumatoid arthritis and controls. The Journal of rheumatology 1995;22(4):639–643. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
