

Role of Renal Replacement Therapy During the Peri-Transplant Period of Heart Transplantation
- PMID: 33230094
- PMCID: PMC7697654
- DOI: 10.12659/AOT.925648
Role of Renal Replacement Therapy During the Peri-Transplant Period of Heart Transplantation
Abstract
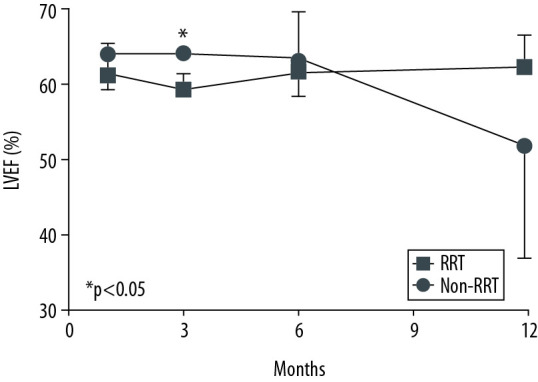
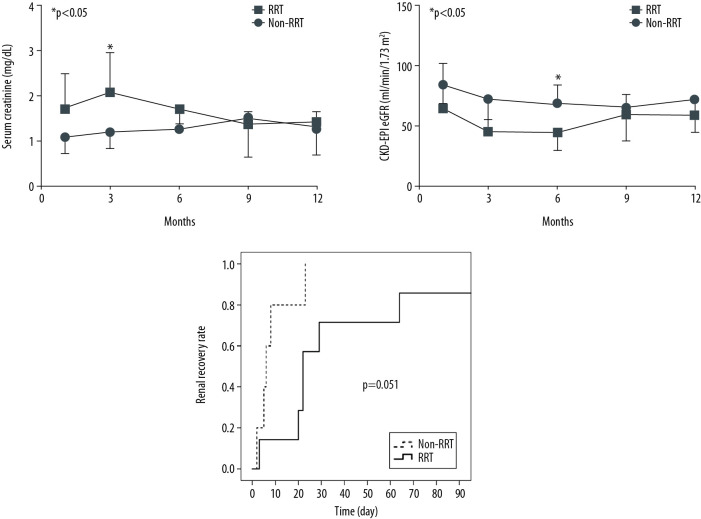
BACKGROUND Heart transplantation (HT) is the most useful treatment modality for heart failure. Although several studies have reported the impact of acute kidney injury (AKI) on clinical outcomes after transplantation, little is known about the impact of peri-transplant renal replacement therapy (RRT) on clinical outcomes. We compared the clinical outcomes according to RRT use status among patients with AKI during the peri-transplant period. MATERIAL AND METHODS The medical records of 21 patients who underwent HT from January 2006 to May 2019 were reviewed. We assessed the heart failure cause, comorbidities, immunosuppressant type, requirement for extracorporeal membrane oxygenation, AKI incidence, and cardiac and renal functions over time. The patients were divided into 3 groups: those without AKI (non-AKI group, n=6), those who underwent perioperative RRT (RRT group, n=10), and those who did not undergo RRT (non-RRT group, n=5). RESULTS The most common cause of HT was dilated cardiomyopathy (52.4%). Fifteen patients (71.4%) experienced AKI during the peri-transplant period. Among them, 9 (90%) in the RRT group underwent continuous RRT and only 1 (10%) underwent intermittent hemodialysis. Until 6 months after HT, the renal function of the RRT group was worse than that of the non-RRT group (estimated glomerular filtration rate 44.2 vs. 69.2 mL/min/1.73 m2, P=0.015), but the differences dissipated by 9 months. Finally, all patients, even in the RRT group, withdrew from dialysis. CONCLUSIONS RRT during the peri-transplant period in HT may be a good bridge therapy for renal function recovery in patients with cardiorenal AKI.
Conflict of interest statement
None.
Figures
References
-
- McCartney SL, Patel C, Del Rio JM. Long-term outcomes and management of the heart transplant recipient. Best Pract Res Clin Anaesthesiol. 2017;31:237–48. - PubMed
-
- Stehlik J, Kobashigawa J, Hunt SA, et al. Honoring 50 years of clinical heart transplantation in circulation: In-depth state-of-the-art review. Circulation. 2018;137:71–87. - PubMed
-
- Ronco C, Bellasi A, Di Lullo L. Cardiorenal syndrome: An overview. Adv Chronic Kidney Dis. 2018;25:382–90. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
