

Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: a retrospective cohort study
- PMID: 33230710
- PMCID: PMC7682692
- DOI: 10.1186/s13613-020-00775-4
Ventilator-associated pneumonia in patients with SARS-CoV-2-associated acute respiratory distress syndrome requiring ECMO: a retrospective cohort study
Abstract
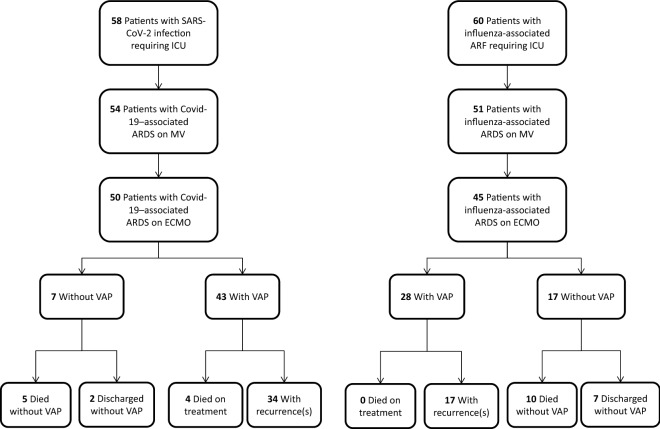
Background: The data on incidence, clinical presentation, and outcomes of ventilator-associated pneumonia (VAP) in patients with severe coronavirus disease 2019 (COVID-19) pneumonia requiring mechanical ventilation (MV) are limited. We performed this retrospective cohort study to assess frequency, clinical characteristics, responsible pathogens, and outcomes of VAP in patients COVID-19 pneumonia requiring MV between March 12th and April 24th, 2020 (all had RT-PCR-confirmed SARS-CoV-2 infection). Patients with COVID-19-associated acute respiratory distress syndrome (ARDS) requiring ECMO were compared with an historical cohort of 45 patients with severe influenza-associated ARDS requiring ECMO admitted to the same ICU during the preceding three winter seasons.
Results: Among 50 consecutive patients with Covid-19-associated ARDS requiring ECMO included [median (IQR) age 48 (42-56) years; 72% male], 43 (86%) developed VAP [median (IQR) MV duration before the first episode, 10 (8-16) days]. VAP-causative pathogens were predominantly Enterobacteriaceae (70%), particularly inducible AmpC-cephalosporinase producers (40%), followed by Pseudomonas aeruginosa (37%). VAP recurred in 34 (79%) patients and 17 (34%) died. Most recurrences were relapses (i.e., infection with the same pathogen), with a high percentage occurring on adequate antimicrobial treatment. Estimated cumulative incidence of VAP, taking into account death and extubation as competing events, was significantly higher in Covid-19 patients than in influenza patients (p = 0.002). Despite a high P. aeruginosa-VAP rate in patients with influenza-associated ARDS (54%), the pulmonary infection recurrence rate was significantly lower than in Covid-19 patients. Overall mortality was similar for the two groups.
Conclusions: Patients with severe Covid-19-associated ARDS requiring ECMO had a very high late-onset VAP rate. Inducible AmpC-cephalosporinase-producing Enterobacteriaceae and Pseudomonas aeruginosa frequently caused VAP, with multiple recurrences and difficulties eradicating the pathogen from the lung.
Keywords: ARDS; Coronavirus; Covid-19; ECMO; Enterobacteriaceae; Ventilator-associated pneumonia.
Conflict of interest statement
C.-E. L. has served as consultant for Bayer Healthcare, Carmat and Thermo Fisher Brahms, and received lecture fees from MSD, Aerogen and BioMérieux, outside the submitted work. The other authors have no conflicts of interest to declare in relationship to this manuscript.
Figures

References
LinkOut - more resources
Full Text Sources
Miscellaneous
