

Diabetes, metformin and glucose lowering therapies after myocardial infarction: Insights from the SWEDEHEART registry
- PMID: 33231125
- PMCID: PMC7919225
- DOI: 10.1177/1479164120973676
Diabetes, metformin and glucose lowering therapies after myocardial infarction: Insights from the SWEDEHEART registry
Abstract
Objective: To explore real-life use of glucose lowering drugs and prognosis after acute myocardial infarction (AMI) with a special focus on metformin.
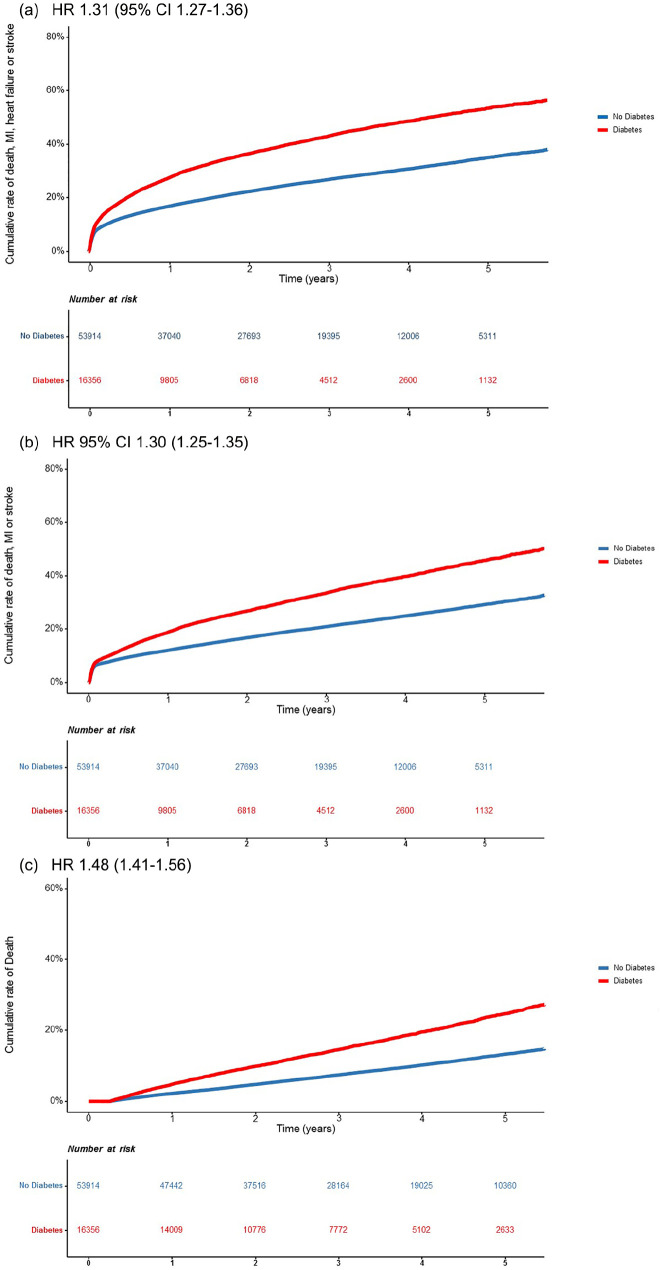
Methods: Patients (n = 70270) admitted for AMI 2012-2017 were stratified by diabetes status and glucose lowering treatment and followed for mortality and MACE+ (AMI, heart failure (HF), stroke, mortality) until end of 2017 (mean follow-up time 3.4 ± 1.4 years) through linkage with national registries and SWEDEHEART. Hazard ratios (HR) were calculated in adjusted Cox proportional hazard regression models.
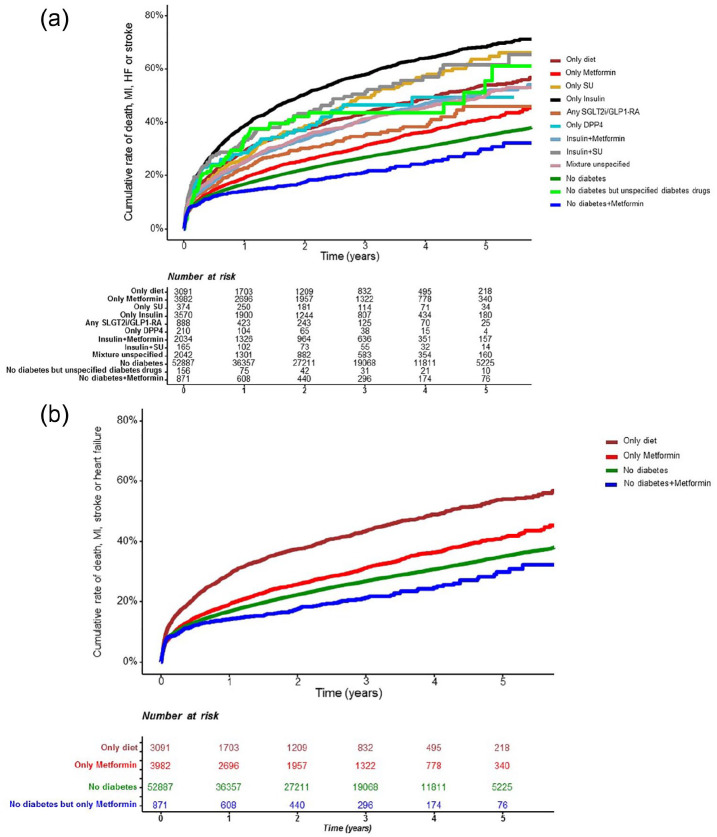
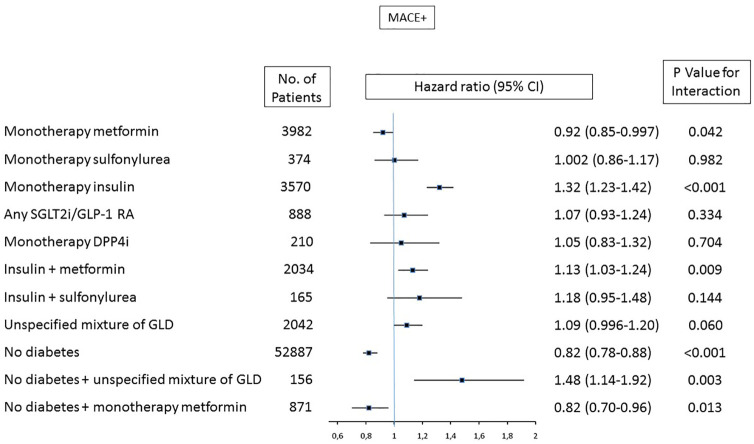
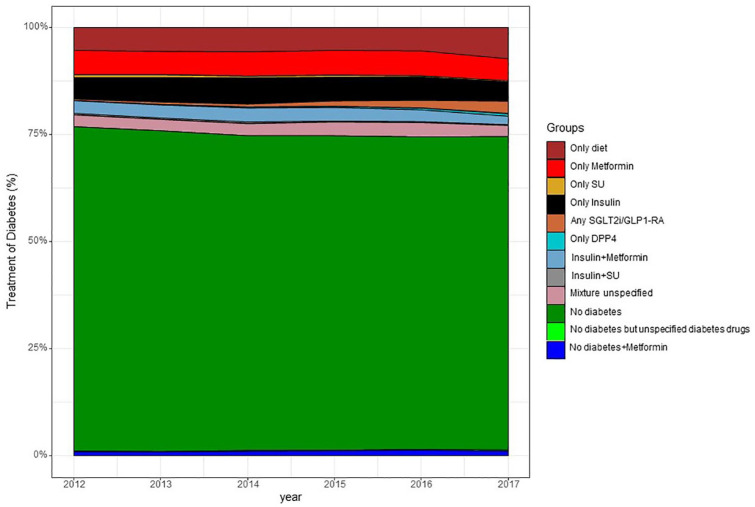
Results: Mean age was 68 ± 11 years and 70% were male. Of patients with diabetes (n = 16356; 23%), a majority had at least one glucose lowering drug (81%) of whom 51% had metformin (24% monotherapy), 43% insulin and a minority any SGLT2i/GLP-1 RA (5%). Adjusted HR for patients with versus without diabetes was 1.31 (95% CI 1.27-1.36) for MACE+ and 1.48 (1.41-1.56) for mortality. Adjusted HR for MACE+ for diabetes patients on metformin was 0.92 (0.85-0.997), p = 0.042 compared to diet treated diabetes.
Conclusion: Diabetes still implies a high complication risk after AMI. Metformin and insulin were the most common treatment used in almost half of the diabetes population. Furthermore, patients treated with metformin had a lower cardiovascular risk after AMI and needs to be confirmed in prospective controlled trials.
Keywords: Diabetes; glucose lowering treatment; metformin; myocardial infarction; outcome.
Conflict of interest statement
Figures
References
-
- Ritsinger V, Saleh N, Lagerqvist B, et al.. High event rate after a first percutaneous coronary intervention (PCI) in patients with diabetes results from the Swedish coronary angiography and angioplasty registry (SCAAR). Circ Cardiovasc Interv 2015; 8: e00232. - PubMed
-
- Ritsinger V, Tanoglidi E, Malmberg K, et al.. Sustained prognostic implications of newly detected glucose abnormalities in patients with: long-term follow-up of the glucose tolerance in patients with acute myocardial infarction cohort. Diab Vasc Dis Res 2015; 12(1): 23−32. - PubMed
-
- Rossello X, Ferreira JP, McMurray JJ, et al.. High-risk myocardial infarction database initiative. Impact of insulin-treated diabetes on cardiovascular outcomes following high-risk myocardial infarction. Eur Heart J Acute Cardiovasc Care 2019; 8(3): 231−241. - PubMed
-
- Zinman B, Wanner C, Lachin JM, et al.. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117−2128. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
