

Randomized clinical trial of pembrolizumab vs chemotherapy for previously untreated Chinese patients with PD-L1-positive locally advanced or metastatic non-small-cell lung cancer: KEYNOTE-042 China Study
- PMID: 33231285
- PMCID: PMC8048589
- DOI: 10.1002/ijc.33399
Randomized clinical trial of pembrolizumab vs chemotherapy for previously untreated Chinese patients with PD-L1-positive locally advanced or metastatic non-small-cell lung cancer: KEYNOTE-042 China Study
Abstract
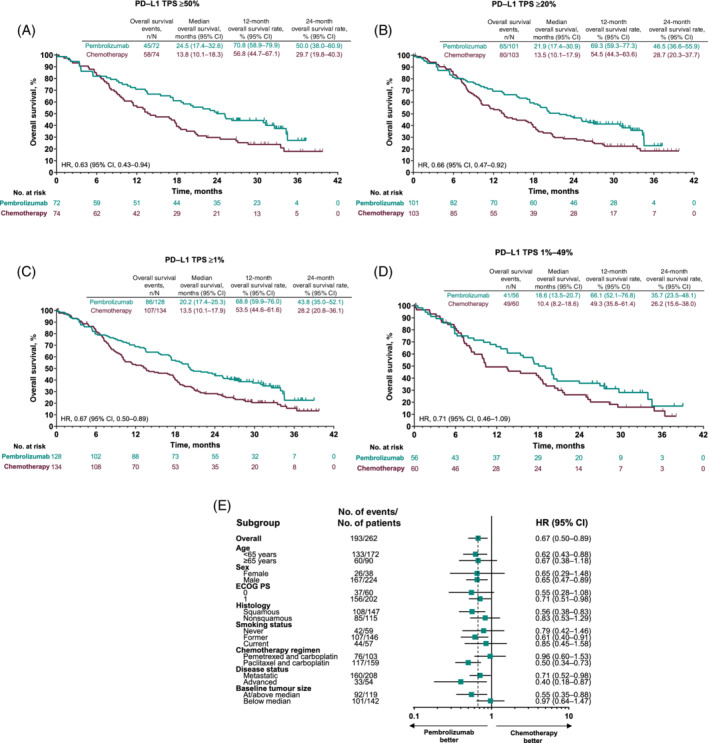
In the global KEYNOTE-042 study (Clinicaltrials.gov, NCT02220894), pembrolizumab significantly improved overall survival (OS) vs chemotherapy in patients with previously untreated programmed death ligand 1 (PD-L1)-positive locally advanced/metastatic non-small-cell lung cancer (NSCLC) without EGFR/ALK alterations. We present results from patients in KEYNOTE-042 enrolled from China in the global or extension study (NCT03850444; protocol identical to global study). Patients were randomized 1:1 (stratified by ECOG performance status 0 vs 1, squamous vs nonsquamous histology and PD-L1 tumor proportion score [TPS] ≥50% vs 1%-49%) to 35 cycles of pembrolizumab 200 mg every 3 weeks (Q3W) or investigator's choice of 4 to 6 cycles of carboplatin plus paclitaxel or pemetrexed Q3W with optional pemetrexed maintenance for nonsquamous tumors. Primary endpoints were OS in patients with PD-L1 TPS ≥50%, ≥20% or ≥1%. Two hundred sixty-two patients (pembrolizumab, n = 128; chemotherapy, n = 134) were enrolled from China. At data cutoff (February 21, 2020; median follow-up, 33.0 [range, 25.6-41.9] months), pembrolizumab was shown to improve OS vs chemotherapy in patients with PD-L1 TPS ≥50% (hazard ratio [95% CI], 0.63 [0.43-0.94]), TPS ≥20% (0.66 [0.47-0.92]) and TPS ≥1% (0.67 [0.50-0.89]). Grade 3 to 5 treatment-related adverse events occurred less frequently with pembrolizumab vs chemotherapy (19.5% vs 68.8%). In 22 patients who completed 35 cycles of pembrolizumab, objective response rate was 77.3% and median duration of response was 27.6 months. Consistent with the global KEYNOTE-042 study, pembrolizumab improved OS vs chemotherapy in this study of Chinese patients with locally advanced/metastatic NSCLC and PD-L1 TPS ≥1%, supporting first-line pembrolizumab monotherapy for PD-L1-positive advanced/metastatic NSCLC in China.
Keywords: chemotherapy; non-small-cell lung cancer; pembrolizumab; programmed death ligand 1.
© 2020 The Authors. International Journal of Cancer published by John Wiley & Sons Ltd on behalf of UICC.
Conflict of interest statement
Y‐L Wu has received speaker fees from AstraZeneca, BMS, Boehringer Ingelheim, Eli Lilly, Hengrui, MSD, Roche, Pfizer and Sanofi; and research funding to the institution from AstraZeneca, BMS and Pfizer. L Zhang (Guangzhou) has received research grants from Hengrui, BMS and Innovent Biologics. Q Zhou has received honoraria from AstraZeneca and Roche. CC Zhou has received honoraria from Boehringer Ingelheim, Eli Lilly, Hengrui, MSD, Sanofi, F. Hoffmann‐La Roche Ltd. and Qilu. T Dang and S Sadowski are employees of Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA. DA Kush is an employee of and stockholder in Merck & Co., Inc., Kenilworth, NJ, USA. Y Zhou and B Li are employees of MSD China. T Mok has received grants or research support from AstraZeneca, Boehringer Ingelheim, Bristol‐Myers Squibb, Clovis Oncology, Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, Novartis, Pfizer, Roche/Genentech, SFJ Pharmaceuticals, Taiho and XCovery; honoraria and/or speakers' fees from Amoy Diagnostics Co. Ltd., AstraZeneca, Boehringer Ingelheim, Bristol‐Myers Squibb, Eli Lilly, InMed Medical Communication, Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, Merck Serono, Novartis, Pfizer, PRIME Oncology, Roche/Genentech, SFJ Pharmaceuticals, Taiho, Virtus Medical Group, and Takeda Oncology; is a stockholder in Biolidics Ltd., Hutchison ChiMed, Loxo‐Oncology, OrigiMed. and Sanomics Ltd.; and has served as an advisory board member and/or consultant for ACEA Biosciences Inc., Alpha Biopharma Co., Ltd., AstraZeneca, Bayer, Daiichi Sankyo, Incyte Corporation, Boehringer Ingelheim, Bristol‐Myers Squibb, Celgene, Cirina, CStone Pharmaceuticals, Eli Lilly, Fishawack Facilitate Ltd., geneDecode Co. Ltd. Hengrui Therapeutics, Ignyta Inc., IQVIA, Janssen, Loxo‐Oncology, Merck Serono, Merck Sharp & Dohme Corp., a subsidiary of Merck & Co., Inc., Kenilworth, NJ, USA, MoreHealth, Novartis, OncoGenex Technologies Inc., OrigiMed, Pfizer, Roche/Genentech, Sanofi‐Aventis, SFJ Pharmaceuticals, Takeda, Vertex Pharmaceuticals, Virtus Medical Group, Biolidics Ltd. and Yuhan Corp; and has leadership positions with ASCO, CSCO and IASLC.
L Zhang (Beijing), Y Fan, JY Zhou, W Li, CP Hu, GY Chen and X Zhang have nothing to disclose.
Figures
References
-
- Shigematsu H, Gazdar AF. Somatic mutations of epidermal growth factor receptor signaling pathway in lung cancers. Int J Cancer. 2006;118:257‐262. - PubMed
-
- Soo RA, Loh M, Mok TS, et al. Ethnic differences in survival outcome in patients with advanced stage non‐small cell lung cancer: results of a meta‐analysis of randomized controlled trials. J Thorac Oncol. 2011;6:1030‐1038. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
