

Association of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Blockers With Severity of COVID-19: A Multicenter, Prospective Study
- PMID: 33231487
- PMCID: PMC8010897
- DOI: 10.1177/1074248420976279
Association of Angiotensin-Converting Enzyme Inhibitors and Angiotensin II Blockers With Severity of COVID-19: A Multicenter, Prospective Study
Abstract
Background: Speculations whether treatment with angiotensin-converting enzyme inhibitors (ACE-I) or angiotensin II receptor blockers (ARB) predisposes to severe coronavirus disease 2019 (COVID-19) or worsens its outcomes. This study assessed the association of ACE-I/ARB therapy with the development of severe COVID-19.
Methods: This multi-center, prospective study enrolled patients hospitalized for COVID-19 and receiving one or more antihypertensive agents to manage either hypertension or cardiovascular disease. ACE-I/ARB therapy associations with severe COVID-19 on the day of hospitalization, intensive care unit (ICU) admission, mechanical ventilation and in-hospital death on follow-up were tested using a multivariate logistic regression model adjusted for age, obesity, and chronic illnesses. The composite outcome of mechanical ventilation and death was examined using the adjusted Cox multivariate regression model.
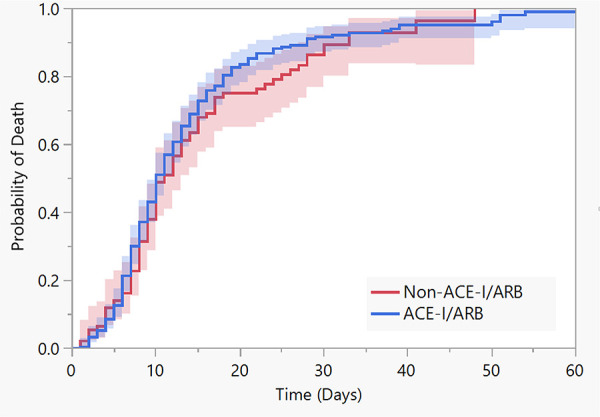
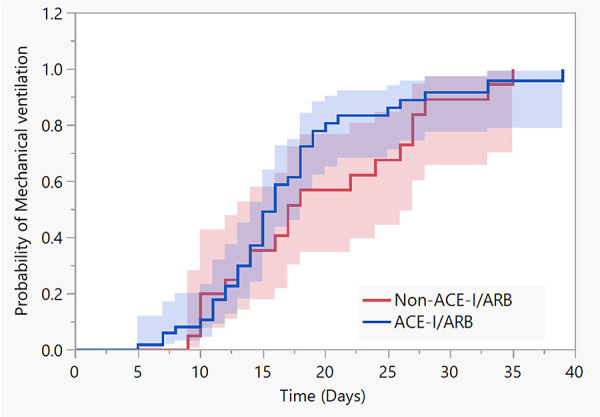
Results: Of 338 enrolled patients, 245 (72.4%) were using ACE-I/ARB on the day of hospital admission, and 197 continued ACE-I/ARB therapy during hospitalization. Ninety-eight (29%) patients had a severe COVID-19, which was not significantly associated with the use of ACE-I/ARB (OR 1.17, 95% CI 0.66-2.09; P = .57). Prehospitalization ACE-I/ARB therapy was not associated with ICU admission, mechanical ventilation, or in-hospital death. Continuing ACE-I/ARB therapy during hospitalization was associated with decreased mortality (OR 0.22, 95% CI 0.073-0.67; P = .008). ACE-I/ARB use was not associated with developing the composite outcome of mechanical ventilation and in-hospital death (HR 0.95, 95% CI 0.51-1.78; P = .87) versus not using ACE-I/ARB.
Conclusion: Patients with hypertension or cardiovascular diseases receiving ACE-I/ARB therapy are not at increased risk for severe COVID-19 on admission to the hospital. ICU admission, mechanical ventilation, and mortality are not associated with ACE-I/ARB therapy. Maintaining ACE-I/ARB therapy during hospitalization for COVID-19 lowers the likelihood of death.
Clinical trial registration: ClinicalTrials.gov, NCT4357535.
Trial registration: ClinicalTrials.gov NCT04357535 NCT04357535.
Keywords: COVID-19; SARS-CoV-2; angiotensin II receptor blockers; angiotensin-converting enzyme inhibitor.
Conflict of interest statement
Figures
Similar articles
-
[Association of hypertension and antihypertensive agents and the severity of COVID-19 pneumonia. A monocentric French prospective study].Ann Cardiol Angeiol (Paris). 2020 Nov;69(5):247-254. doi: 10.1016/j.ancard.2020.09.030. Epub 2020 Sep 29. Ann Cardiol Angeiol (Paris). 2020. PMID: 33039120 Free PMC article. French.
-
Angiotensin-Converting Enzyme Inhibitor and Angiotensin Receptor Blocker Use Associated with Reduced Mortality and Other Disease Outcomes in US Veterans with COVID-19.Drugs. 2022 Jan;82(1):43-54. doi: 10.1007/s40265-021-01639-2. Epub 2021 Dec 16. Drugs. 2022. PMID: 34914085 Free PMC article.
-
RAAS inhibitors are not associated with mortality in COVID-19 patients: Findings from an observational multicenter study in Italy and a meta-analysis of 19 studies.Vascul Pharmacol. 2020 Dec;135:106805. doi: 10.1016/j.vph.2020.106805. Epub 2020 Sep 28. Vascul Pharmacol. 2020. PMID: 32992048 Free PMC article.
-
Effect of continuing the use of renin-angiotensin system inhibitors on mortality in patients hospitalized for coronavirus disease 2019: a systematic review, meta-analysis, and meta-regression analysis.BMC Infect Dis. 2023 Jan 24;23(1):53. doi: 10.1186/s12879-023-07994-7. BMC Infect Dis. 2023. PMID: 36694122 Free PMC article.
-
COVID-19 and arterial hypertension: Hypothesis or evidence?J Clin Hypertens (Greenwich). 2020 Jul;22(7):1120-1126. doi: 10.1111/jch.13925. Epub 2020 Jul 6. J Clin Hypertens (Greenwich). 2020. PMID: 32627330 Free PMC article. Review.
Cited by
-
Evaluating the Role of the Renin-angiotensin System in COVID-19: Implications for ACE Inhibitor and ARB Use During SARS-CoV-2 Infection.J Cell Immunol. 2024;6(6):255-265. doi: 10.33696/immunology.6.213. J Cell Immunol. 2024. PMID: 40417281 Free PMC article.
-
Drugs acting on the renin-angiotensin-aldosterone system (RAAS) and deaths of COVID-19 patients: a systematic review and meta-analysis of observational studies.Egypt Heart J. 2022 Sep 6;74(1):64. doi: 10.1186/s43044-022-00303-8. Egypt Heart J. 2022. PMID: 36068392 Free PMC article.
-
Antihypertensive drug treatment and susceptibility to SARS-CoV-2 infection in human PSC-derived cardiomyocytes and primary endothelial cells.Stem Cell Reports. 2021 Oct 12;16(10):2459-2472. doi: 10.1016/j.stemcr.2021.08.018. Epub 2021 Sep 1. Stem Cell Reports. 2021. PMID: 34525378 Free PMC article.
-
Biologia Futura: is ADAM 17 the reason for COVID-19 susceptibility in hyperglycemic and diabetic patients?Biol Futur. 2021 Sep;72(3):291-297. doi: 10.1007/s42977-021-00092-2. Epub 2021 Jun 8. Biol Futur. 2021. PMID: 34554559 Free PMC article. Review.
-
Renin-Angiotensin Aldosterone System Inhibitors and COVID-19: A Systematic Review and Meta-Analysis Revealing Critical Bias Across a Body of Observational Research.J Am Heart Assoc. 2022 Jun 7;11(11):e025289. doi: 10.1161/JAHA.122.025289. Epub 2022 May 27. J Am Heart Assoc. 2022. PMID: 35624081 Free PMC article.
References
-
- Onder G, Rezza G, Brusaferro S. Case-fatality rate and characteristics of patients dying in relation to COVID-19 in Italy. JAMA. 2020;323(18):1775–1776. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
