

Safety Assessment of a Noninvasive Respiratory Protocol for Adults With COVID-19
- PMID: 33231547
- PMCID: PMC8034674
- DOI: 10.12788/jhm.3548
Safety Assessment of a Noninvasive Respiratory Protocol for Adults With COVID-19
Abstract
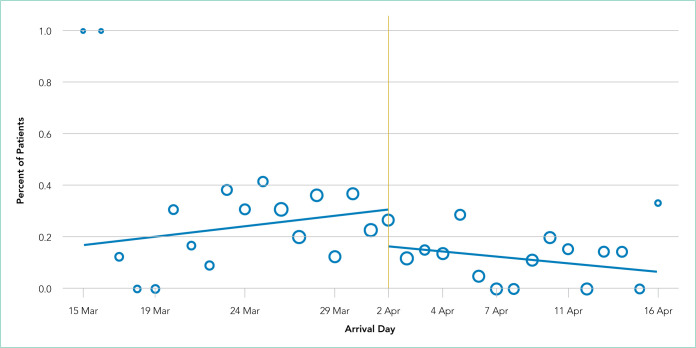
As evidence emerged supporting noninvasive strategies for coronavirus disease 2019 (COVID-19)-related respiratory distress, we implemented a noninvasive COVID-19 respiratory protocol (NCRP) that encouraged high-flow nasal cannula (HFNC) and self-proning across our healthcare system. To assess safety, we conducted a retrospective chart review evaluating mortality and other patient safety outcomes after implementation of the NCRP protocol (April 3, 2020, to April 15, 2020) for adult patients hospitalized with COVID-19, compared with preimplementation outcomes (March 15, 2020, to April 2, 2020). During the study, there were 469 COVID-19 admissions. Fewer patients underwent intubation after implementation (10.7% [23 of 215]), compared with before implementation (25.2% [64 of 254]) (P < .01). Overall, 26.2% of patients died (24% before implementation vs 28.8% after implementation; P = .14). In patients without a do not resuscitate/do not intubate order prior to admission, mortality was 21.8% before implementation vs 21.9% after implementation. Overall, we found no significant increase in mortality following implementation of a noninvasive respiratory protocol that decreased intubations in patients with COVID-19.
Figures
Comment in
-
Implementing Change in the Heat of the Moment.J Hosp Med. 2020 Dec;15(12):768. doi: 10.12788/jhm.3565. J Hosp Med. 2020. PMID: 33284745 Free PMC article. No abstract available.
-
Outcomes of COVID-19 patients treated with noninvasive respiratory support outside-ICU setting: a Portuguese reality.Pulmonology. 2022 Jan-Feb;28(1):59-61. doi: 10.1016/j.pulmoe.2021.09.002. Epub 2021 Oct 2. Pulmonology. 2022. PMID: 34702677 Free PMC article. No abstract available.
References
-
- Cummings MJ, Baldwin MR, Abrams D, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. 2020;395(10239):1763–1770. doi: 10.1016/s0140-6736(20)31189-2. doi: 10.1016/S0140-6736(20)31189-2. - DOI - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
