

Androgen Signaling Regulates SARS-CoV-2 Receptor Levels and Is Associated with Severe COVID-19 Symptoms in Men
- PMID: 33232663
- PMCID: PMC7670929
- DOI: 10.1016/j.stem.2020.11.009
Androgen Signaling Regulates SARS-CoV-2 Receptor Levels and Is Associated with Severe COVID-19 Symptoms in Men
Abstract
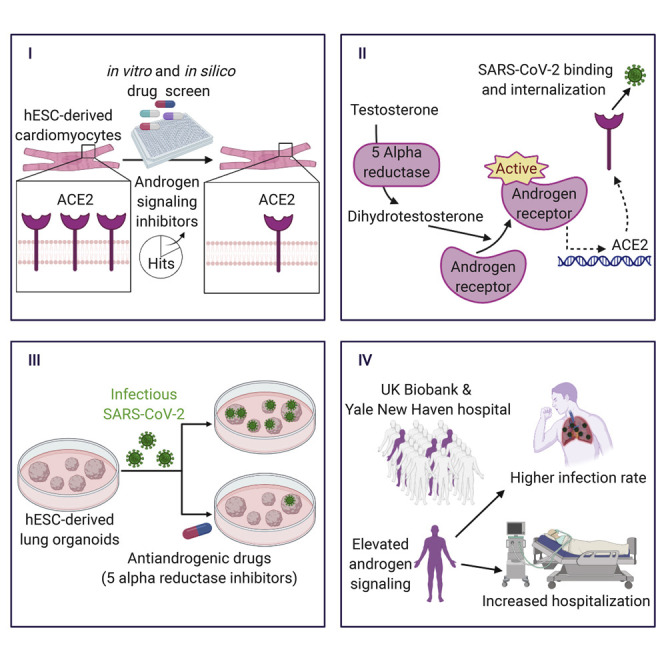
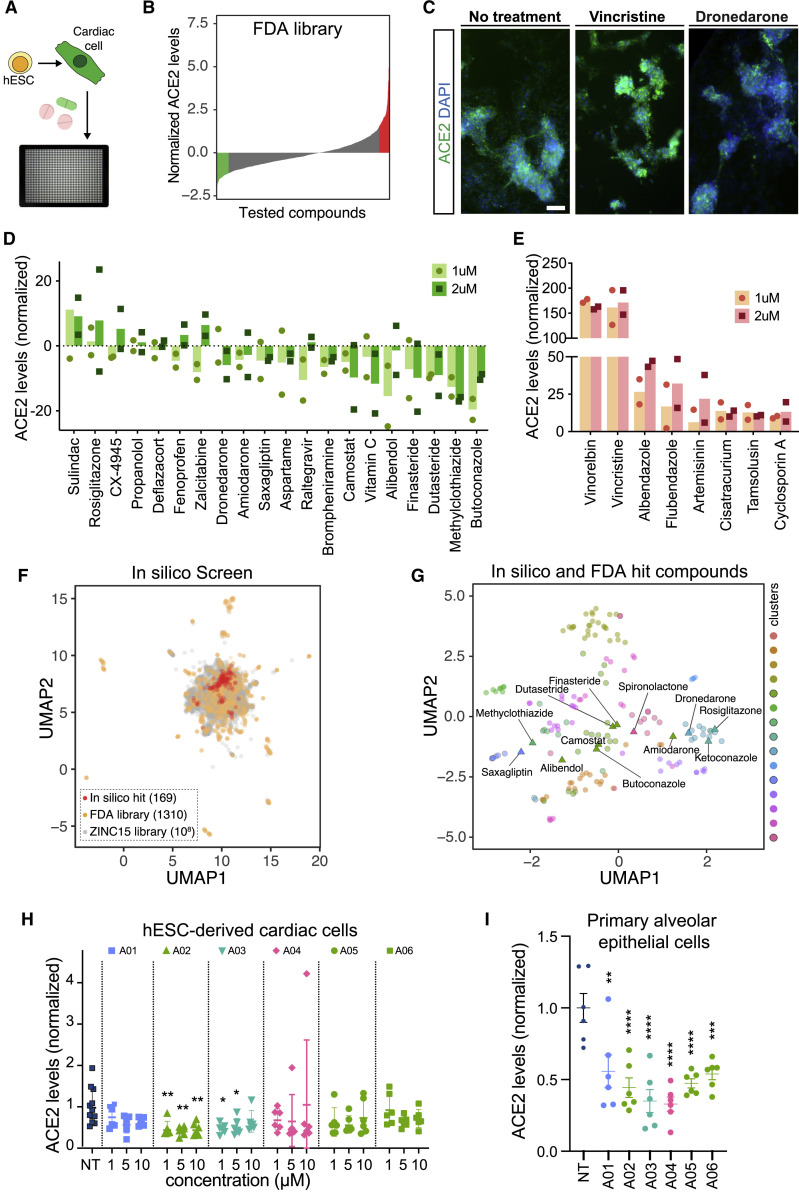
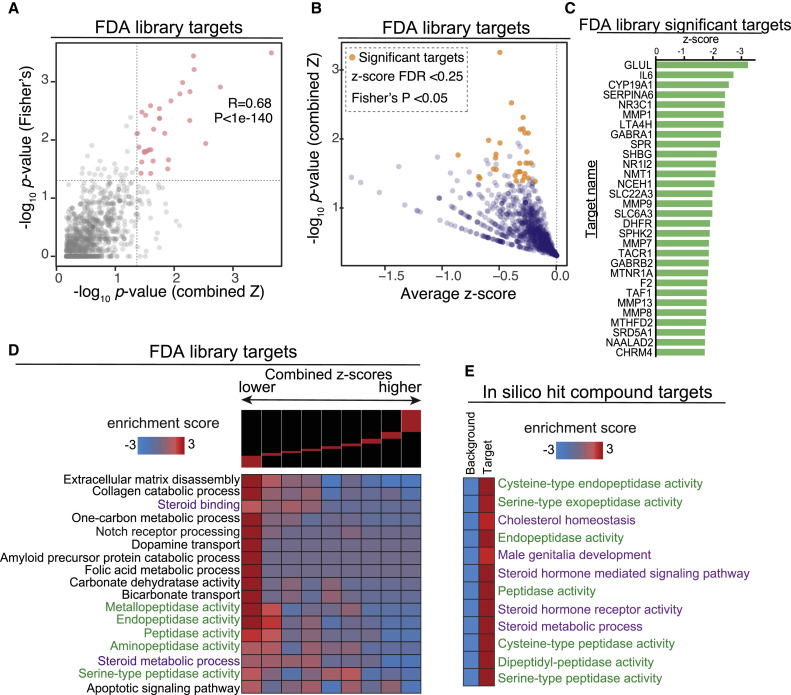
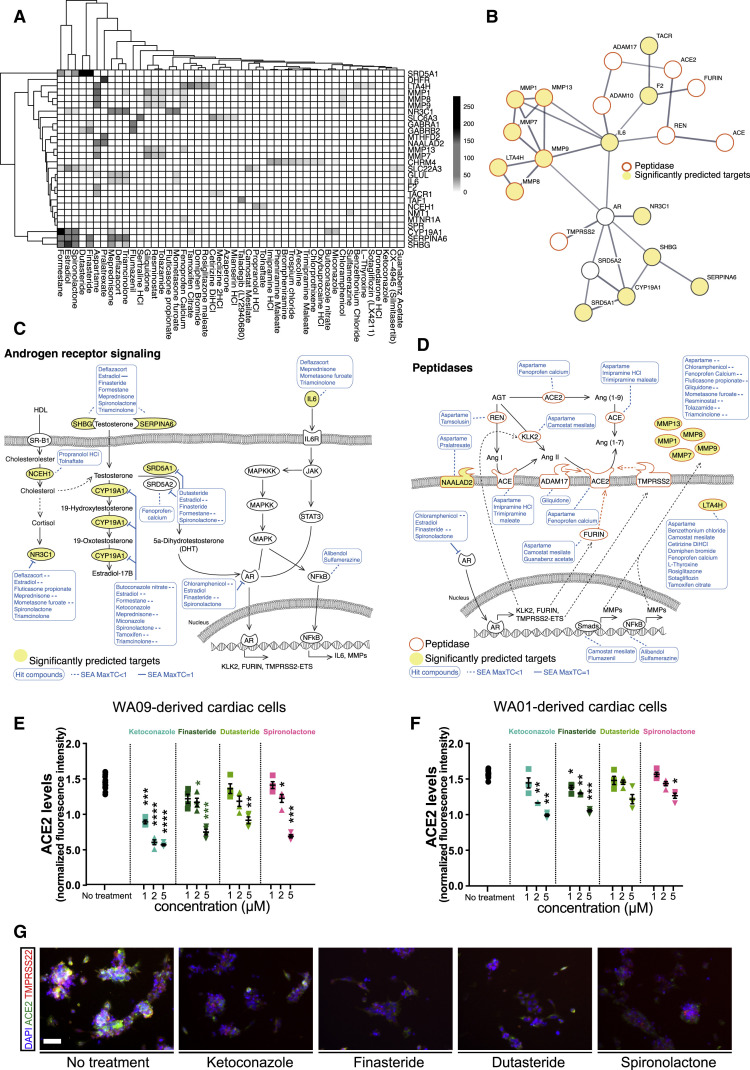
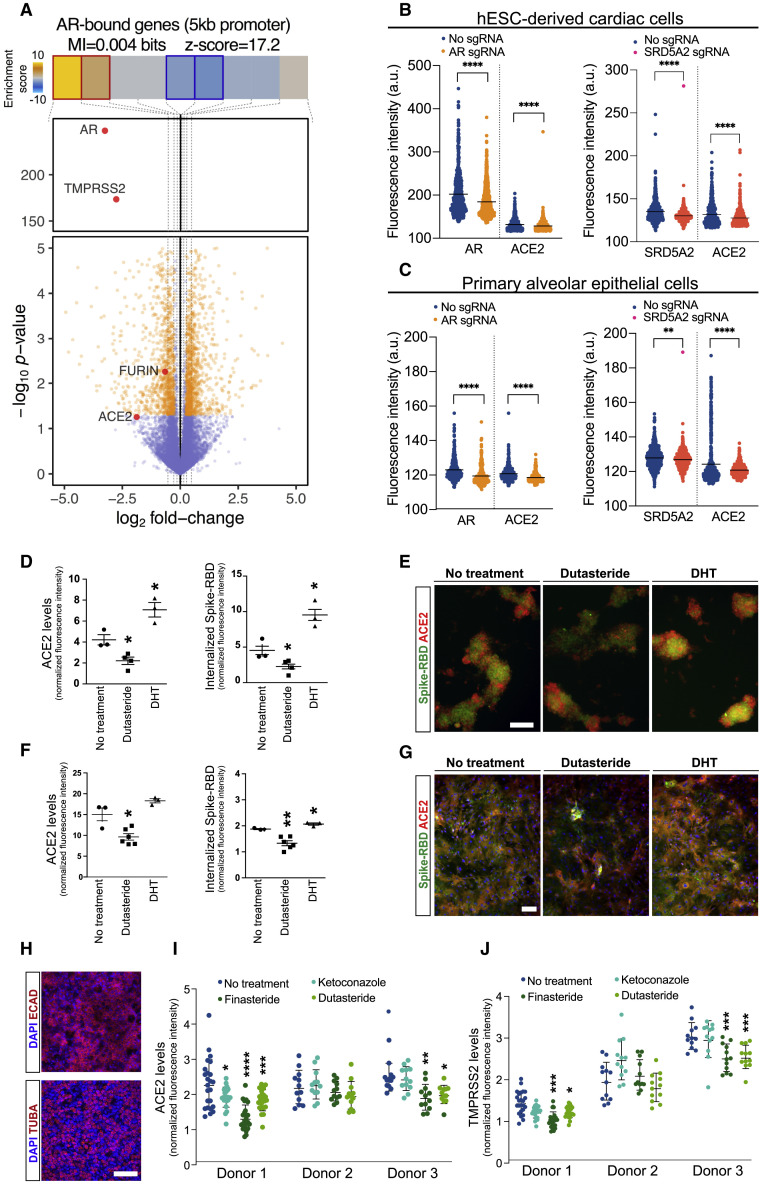
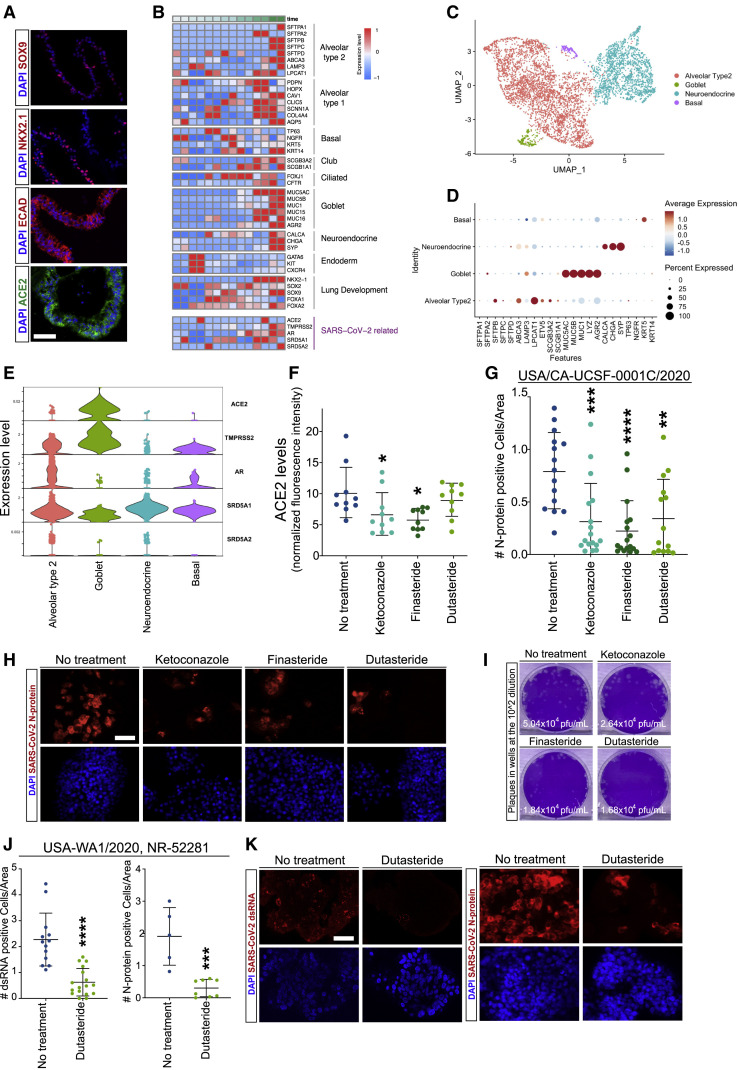
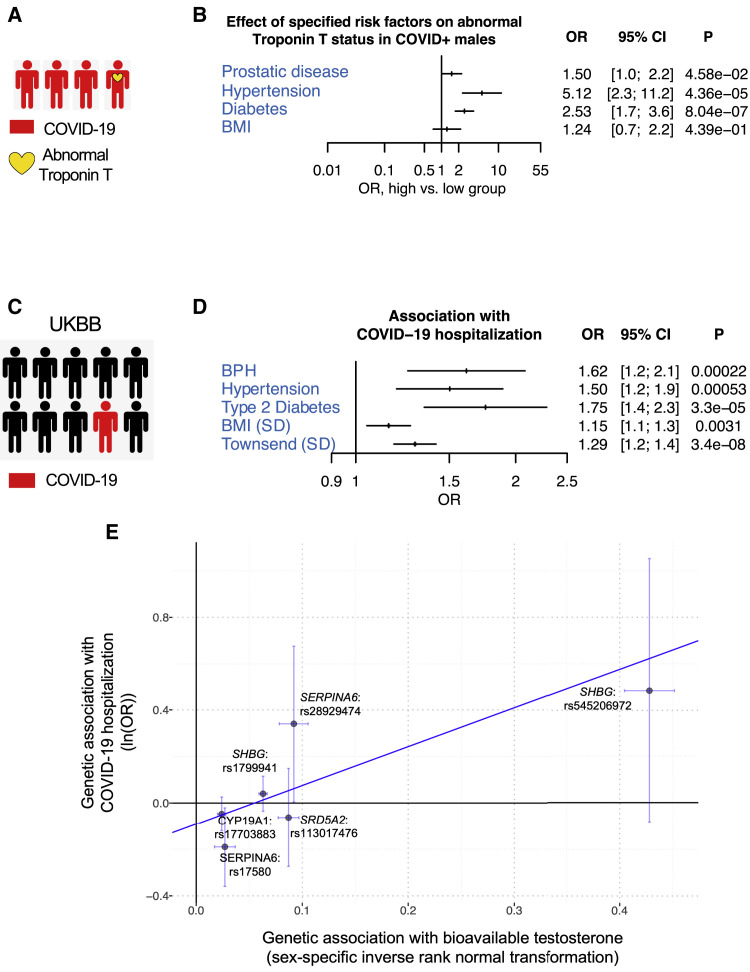
SARS-CoV-2 infection has led to a global health crisis, and yet our understanding of the disease and potential treatment options remains limited. The infection occurs through binding of the virus with angiotensin converting enzyme 2 (ACE2) on the cell membrane. Here, we established a screening strategy to identify drugs that reduce ACE2 levels in human embryonic stem cell (hESC)-derived cardiac cells and lung organoids. Target analysis of hit compounds revealed androgen signaling as a key modulator of ACE2 levels. Treatment with antiandrogenic drugs reduced ACE2 expression and protected hESC-derived lung organoids against SARS-CoV-2 infection. Finally, clinical data on COVID-19 patients demonstrated that prostate diseases, which are linked to elevated androgen, are significant risk factors and that genetic variants that increase androgen levels are associated with higher disease severity. These findings offer insights on the mechanism of disproportionate disease susceptibility in men and identify antiandrogenic drugs as candidate therapeutics for COVID-19.
Keywords: 5-alpha reductase inhibitors; ACE2 regulation; COVID-19 risk factors; COVID-19 sex bias; SARS-CoV-2 infection model; deep learning; drug re-purposing; hPSC-based disease modeling; high content screening; virtual drug screen.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Interests P.N. receives grants from Apple, Amgen, and Boston Scientific, and personal fees from Apple and Blackstone Life Sciences, all outside the submitted work. F.F. receives grants from Takeda Pharmaceuticals on projects outside of the submitted work.
Figures
Update of
-
Androgen Regulates SARS-CoV-2 Receptor Levels and Is Associated with Severe COVID-19 Symptoms in Men.bioRxiv [Preprint]. 2020 May 15:2020.05.12.091082. doi: 10.1101/2020.05.12.091082. bioRxiv. 2020. Update in: Cell Stem Cell. 2020 Dec 3;27(6):876-889.e12. doi: 10.1016/j.stem.2020.11.009. PMID: 32511360 Free PMC article. Updated. Preprint.
References
Publication types
MeSH terms
Substances
Grants and funding
- R01 CA240984/CA/NCI NIH HHS/United States
- DP1 DA038043/DA/NIDA NIH HHS/United States
- T32 HD007470/HD/NICHD NIH HHS/United States
- R01 HL148050/HL/NHLBI NIH HHS/United States
- DP2 NS116769/NS/NINDS NIH HHS/United States
- R01 GM123977/GM/NIGMS NIH HHS/United States
- F30 HL149180/HL/NHLBI NIH HHS/United States
- F32 GM133118/GM/NIGMS NIH HHS/United States
- R01 HL148565/HL/NHLBI NIH HHS/United States
- R35 HL145235/HL/NHLBI NIH HHS/United States
- U19 AI077439/AI/NIAID NIH HHS/United States
- R01 DK121169/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
