

One-Stage Extension Shortening Osteotomy for Syndromic Camptodactyly
- PMID: 33233749
- PMCID: PMC7699896
- DOI: 10.3390/jcm9113731
One-Stage Extension Shortening Osteotomy for Syndromic Camptodactyly
Abstract
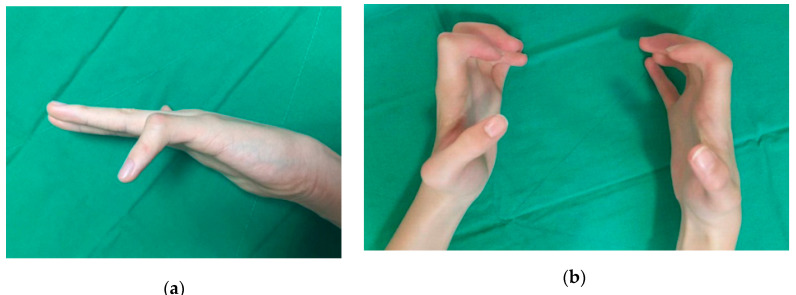
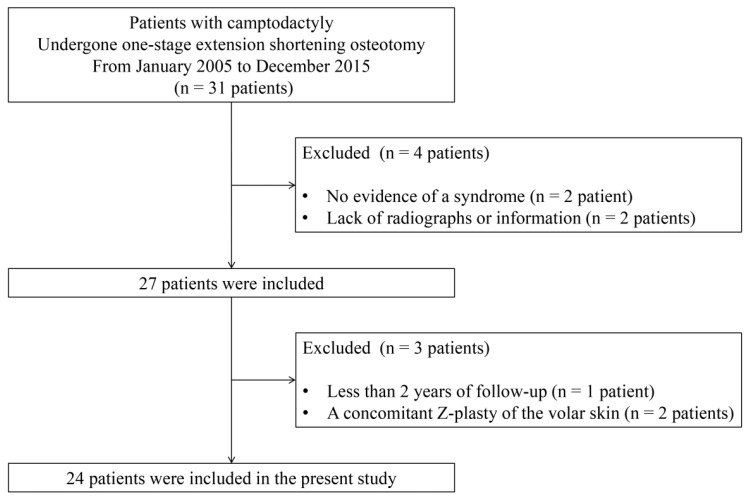
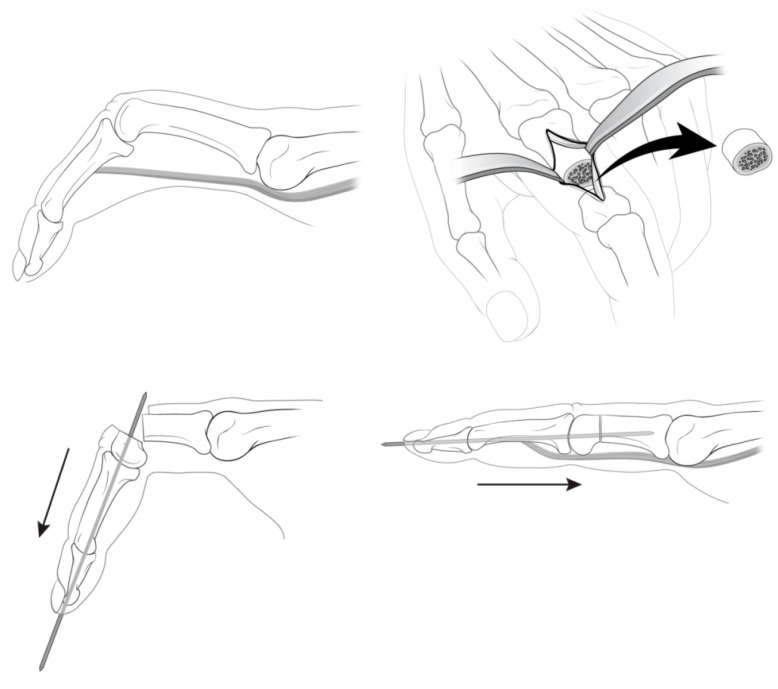
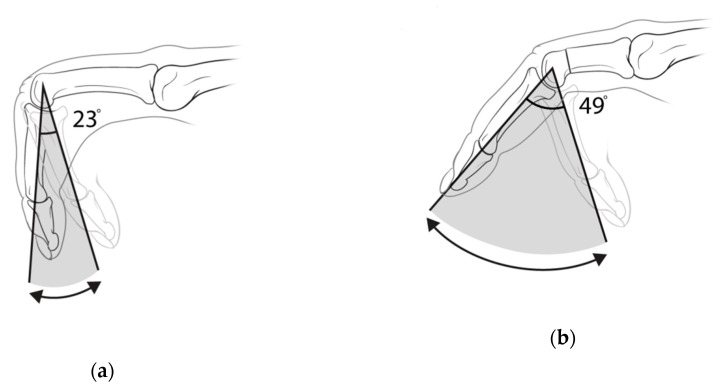
Syndromic camptodactyly often affects multiple fingers, and severe deformities are common compared to idiopathic camptodactyly. This study aimed to evaluate the use of a one-stage extension shortening osteotomy of the proximal phalanx for patients with syndromic camptodactyly without tendon surgery. Forty-nine cases of syndromic camptodactyly were included. Forty fingers (81.6%) were associated with arthrogryposis multiplex congenita, and nine (18.4%) with other syndromes. Six fingers presented with a moderate form (30° to 60°) of camptodactyly, whereas 43 fingers manifested the severe form (>60°). The mean age at the time of surgery was 8.5 years, and the patients were followed for a mean of 3.9 years. The mean length of the shortening of the proximal phalanx was 4.9 mm, which averaged 17.8% of the proximal phalanx's original preoperative length. The mean operative time was 25.8 min, and the PIP joint was fixed using Kirschner wires with an average flexion position of 7.6°. The mean flexion contracture improved from 76° preoperatively to 41° postoperatively. The mean preoperative active arc of motion was 23°, which improved to 49° postoperatively. A one-stage extension shortening osteotomy is a straightforward and effective technique for the improvement of finger function through the indirect lengthening of volar structures without the flexor tendon lengthening. The osteotomy could simultaneously correct bony abnormalities. This simple procedure is especially suitable for surgery on multiple fingers in patients with syndromic camptodactyly.
Keywords: camptodactyly; children; finger; osteotomy.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures

Similar articles
-
Early Results of Surgical Management of Camptodactyly.J Pediatr Orthop. 2017 Jul/Aug;37(5):e317-e320. doi: 10.1097/BPO.0000000000000967. J Pediatr Orthop. 2017. PMID: 28277466
-
[Surgical treatment of camptodactyly].Ann Chir Main Memb Super. 1995;14(6):264-71. doi: 10.1016/s0753-9053(05)80405-3. Ann Chir Main Memb Super. 1995. PMID: 8679338 French.
-
Camptodactyly.J Hand Surg Asian Pac Vol. 2024 Dec;29(6):547-553. doi: 10.1142/S2424835524300032. Epub 2024 Nov 14. J Hand Surg Asian Pac Vol. 2024. PMID: 39544035 Review.
-
Long-term outcome following carpal wedge osteotomy in the arthrogrypotic patient.J Bone Joint Surg Am. 2013 Oct 16;95(20):e150. doi: 10.2106/JBJS.L.01122. J Bone Joint Surg Am. 2013. PMID: 24132365
-
The anatomy and treatment of camptodactyly of the small finger.J Hand Surg Am. 1992 Jan;17(1):35-44. doi: 10.1016/0363-5023(92)90110-b. J Hand Surg Am. 1992. PMID: 1538110 Review.
Cited by
-
Camptodactyly: From Embryological Basis to Surgical Treatment.Medicina (Kaunas). 2023 May 17;59(5):966. doi: 10.3390/medicina59050966. Medicina (Kaunas). 2023. PMID: 37241199 Free PMC article.
References
LinkOut - more resources
Full Text Sources
