

The Diagnostic Performance of Interleukin-6 and C-Reactive Protein for Early Identification of Neonatal Sepsis
- PMID: 33233806
- PMCID: PMC7699903
- DOI: 10.3390/diagnostics10110978
The Diagnostic Performance of Interleukin-6 and C-Reactive Protein for Early Identification of Neonatal Sepsis
Abstract
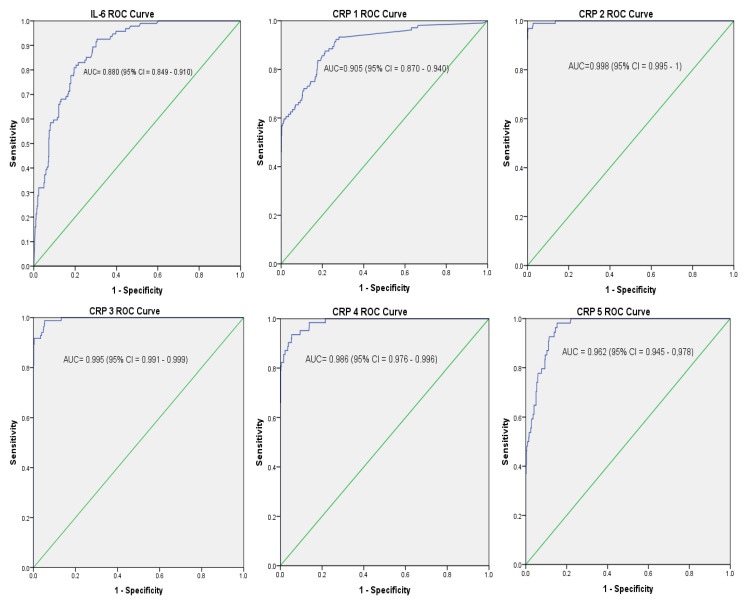
Interleukin-6 (IL-6) and C-reactive protein (CRP) are being used for diagnosis of sepsis. However, studies have reported varying cut-off levels and diagnostic performance. This study aims to investigate the optimal cut-off levels and performance of IL-6 and CRP for the diagnosis of neonatal sepsis. The study was conducted at the University Hospital of Leipzig, Germany from November 2012 to June 2020. A total of 899 neonates: 104 culture proven sepsis, 160 clinical sepsis, and 625 controls were included. Blood culture was performed using BacT/ALERT 3D system. IL-6 and CRP were analyzed by electrochemiluminescent immunoassay and immunoturbidimetric assay, respectively. Data were analyzed using SPSS 20 statistical software. Among neonates with proven sepsis, the optimal cut-off value of IL-6 was 313.5 pg/mL. The optimal cut-off values for CRP in 5 days serial measurements (CRP1, CRP2, CRP3, CRP4, and CRP5) were 2.15 mg/L, 8.01 mg/L, 6.80 mg/L, 5.25 mg/L, and 3.72 mg/L, respectively. IL-6 showed 73.1% sensitivity, 80.2% specificity, 37.6% PPV, and 94.8% NPV. The highest performance of CRP was observed in the second day with 89.4% sensitivity, 97.3% specificity, 94.5% PPV, and 98.3% NPV. The combination of IL-6 and CRP showed increase in sensitivity with decrease in specificity. In conclusion, this study defines the optimal cut-off values for IL-6 and CRP. The combination of IL-6 and CRP demonstrated increased sensitivity. The CRP 2 at cut-off 8.01 mg/L showed the highest diagnostic performance for identification of culture negative clinical sepsis cases. We recommend the combination of IL-6 (≥313.5 pg/mL) and CRP1 (≥2.15 mg/L) or IL-6 (≥313.5 pg/mL) and CRP2 (≥8.01 mg/L) for early and accurate diagnosis of neonatal sepsis. The recommendation is based on increased sensitivity, that is, to minimize the risk of any missing cases of sepsis. The CRP2 alone at cut-off 8.01 mg/L might be used to identify clinical sepsis cases among culture negative sepsis suspected neonates in hospital settings.
Keywords: C-reactive protein; diagnosis; interleukin-6; neonatal sepsis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
What are the cut-off levels for IL-6 and CRP in neonatal sepsis?J Clin Lab Anal. 2010;24(6):407-12. doi: 10.1002/jcla.20420. J Clin Lab Anal. 2010. PMID: 21089127 Free PMC article.
-
The cut-off levels of procalcitonin and C-reactive protein and the kinetics of mean platelet volume in preterm neonates with sepsis.BMC Pediatr. 2018 Aug 1;18(1):253. doi: 10.1186/s12887-018-1236-2. BMC Pediatr. 2018. PMID: 30068303 Free PMC article.
-
[C-reactive protein concentrations during initial (empiric) treatment of neonatal sepsis].Srp Arh Celok Lek. 2001 May-Jun;129 Suppl 1:17-22. Srp Arh Celok Lek. 2001. PMID: 15637985 Serbian.
-
Reliability of Interleukin-6 Alone and in Combination for Diagnosis of Early Onset Neonatal Sepsis: Systematic Review.Front Pediatr. 2022 Mar 23;10:840778. doi: 10.3389/fped.2022.840778. eCollection 2022. Front Pediatr. 2022. PMID: 35402358 Free PMC article.
-
The combination of procalcitonin and C-reactive protein or presepsin alone improves the accuracy of diagnosis of neonatal sepsis: a meta-analysis and systematic review.Crit Care. 2018 Nov 21;22(1):316. doi: 10.1186/s13054-018-2236-1. Crit Care. 2018. PMID: 30463590 Free PMC article.
Cited by
-
Antibiotic Resistance Patterns of Bacterial Isolates from Neonatal Sepsis Patients at University Hospital of Leipzig, Germany.Antibiotics (Basel). 2021 Mar 19;10(3):323. doi: 10.3390/antibiotics10030323. Antibiotics (Basel). 2021. PMID: 33808878 Free PMC article.
-
Inflammatory Biomarker Profiles in Very Preterm Infants within the Context of Preeclampsia, Chorioamnionitis, and Clinically Diagnosed Postnatal Infection.Pediatr Rep. 2023 Aug 10;15(3):483-493. doi: 10.3390/pediatric15030044. Pediatr Rep. 2023. PMID: 37606448 Free PMC article.
-
LINC02363: a potential biomarker for early diagnosis and treatment of sepsis.BMC Immunol. 2025 Mar 15;26(1):23. doi: 10.1186/s12865-025-00702-x. BMC Immunol. 2025. PMID: 40089725 Free PMC article.
-
Salivary Interleukin-6 and C-Reactive Protein/Mean Platelet Volume Ratio in the Diagnosis of Late-Onset Neonatal Pneumonia.J Immunol Res. 2021 Oct 18;2021:8495889. doi: 10.1155/2021/8495889. eCollection 2021. J Immunol Res. 2021. PMID: 34708133 Free PMC article.
-
Proteomics identifies lipocalin-2 in neonatal inflammation associated with cerebrovascular alteration in mice and preterm infants.iScience. 2023 Jun 27;26(7):107217. doi: 10.1016/j.isci.2023.107217. eCollection 2023 Jul 21. iScience. 2023. PMID: 37496672 Free PMC article.
References
-
- Barnett E.D., Klein J.O. In: Infectious Diseases of the Fetus and Newborn. 6th ed. Remington J.S., Klein J.O., editors. Elsevier Health Sciences; Philadelphia, PA, USA: 2011.
-
- Lemons J.A., Bauer C.R., Oh W., Korones S.B., Papile L.-A., Stoll B.J., Verter J., Temprosa M., Wright L.L., Ehrenkranz R.A., et al. Very Low Birth Weight Outcomes of the National Institute of Child Health and Human Development Neonatal Research Network, January 1995 through December 1996. Pediatrics. 2001;107:e1. doi: 10.1542/peds.107.1.e1. - DOI - PubMed
-
- Calil R., Marba S.T.M., Von Nowakonski A., Tresoldi A.T. Reduction in colonization and nosocomial infection by multiresistant bacteria in a neonatal unit after institution of educational measures and restriction in the use of cephalosporins. Am. J. Infect. Control. 2001;29:133–138. doi: 10.1067/mic.2001.114223. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
