

Physicians' clinical prediction of survival in head and neck cancer patients in the palliative phase
- PMID: 33234115
- PMCID: PMC7687732
- DOI: 10.1186/s12904-020-00682-2
Physicians' clinical prediction of survival in head and neck cancer patients in the palliative phase
Abstract
Background: The prognosis of patients with incurable head and neck cancer (HNC) is a relevant topic. The mean survival of these patients is 5 months but may vary from weeks to more than 3 years. Discussing the prognosis early in the disease trajectory enables patients to make well-considered end-of-life choices, and contributes to a better quality of life and death. However, physicians often are reluctant to discuss prognosis, partly because of the concern to be inaccurate. This study investigated the accuracy of physicians' clinical prediction of survival of palliative HNC patients.
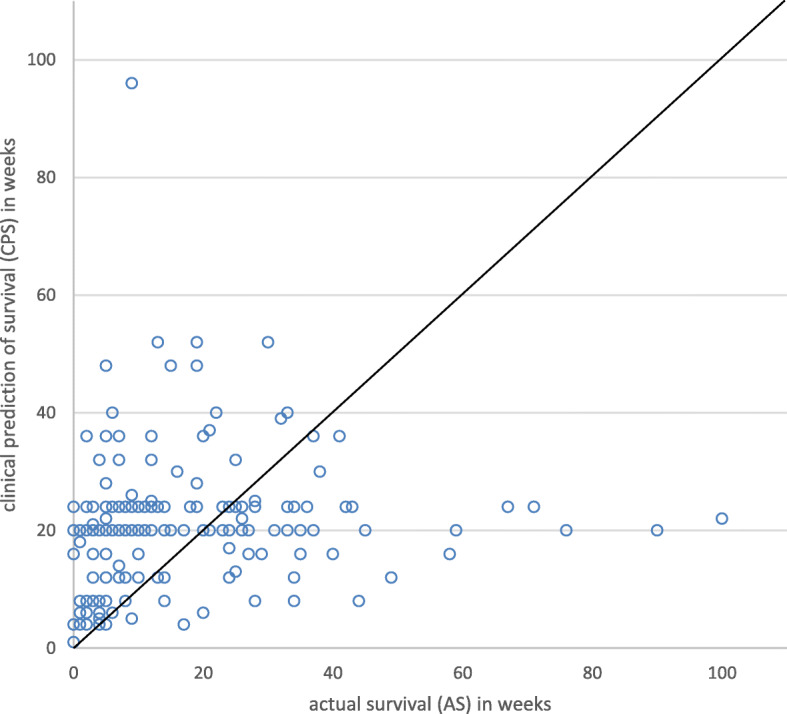
Methods: This study was part of a prospective cohort study in a tertiary cancer center. Patients with incurable HNC diagnosed between 2008 and 2011 (n = 191), and their treating physician were included. Analyses were conducted between July 2018 and February 2019. Patients' survival was clinically predicted by their physician ≤3 weeks after disclosure of the palliative diagnosis. The clinical prediction of survival in weeks (CPS) was based on physicians' clinical assessment of the patient during the outpatient visits. More than 25% difference between the actual survival (AS) and the CPS was regarded as a prediction error. In addition, when the difference between the AS and CPS was 2 weeks or less, this was always considered as correct.
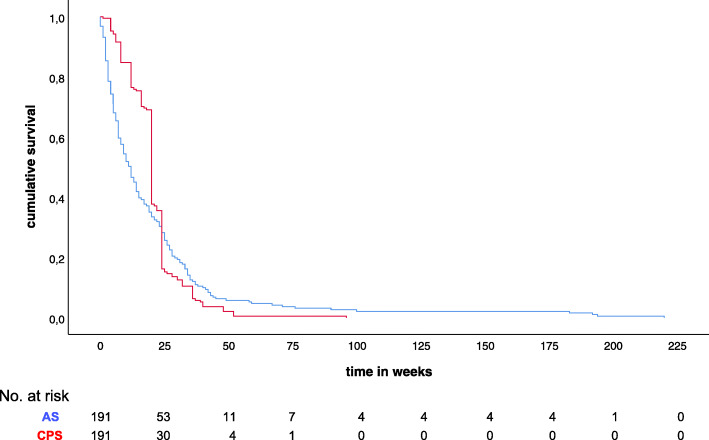
Results: In 59% (n = 112) of cases survival was overestimated. These patients lived shorter than predicted by their physician (median AS 6 weeks, median CPS 20 weeks). In 18% (n = 35) of the cases survival was correctly predicted. The remaining 23% was underestimated (median AS 35 weeks, median CPS 20 weeks). Besides the differences in AS and CPS, no other significant differences were found between the three groups. There was worse accuracy when predicting survival closer to death: out of the 66 patients who survived 6 weeks or shorter, survival was correctly predicted in only eight (12%).
Conclusion: Physicians tend to overestimate the survival of palliative HNC patients. This optimism can result in suboptimal use of palliative and end-of-life care. The future development of a prognostic model that provides more accurate estimates, could help physicians with personalized prognostic counseling.
Keywords: Counseling; Head and neck cancer; Palliative care; Prediction; Prognosis; Survival.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Hoofd-halskanker . Netherlands Comprehensive Cancer Organisation. 2018.
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
