

Robotic versus laparoscopic gastrectomy for gastric cancer: a systematic review and meta-analysis
- PMID: 33234134
- PMCID: PMC7688002
- DOI: 10.1186/s12957-020-02080-7
Robotic versus laparoscopic gastrectomy for gastric cancer: a systematic review and meta-analysis
Abstract
Background: To date, robotic surgery has been widely used worldwide. We conducted a systematic review and meta-analysis to evaluate short-term and long-term outcomes of robotic gastrectomy (RG) in gastric cancer patients to determine whether RG can replace laparoscopic gastrectomy (LG).
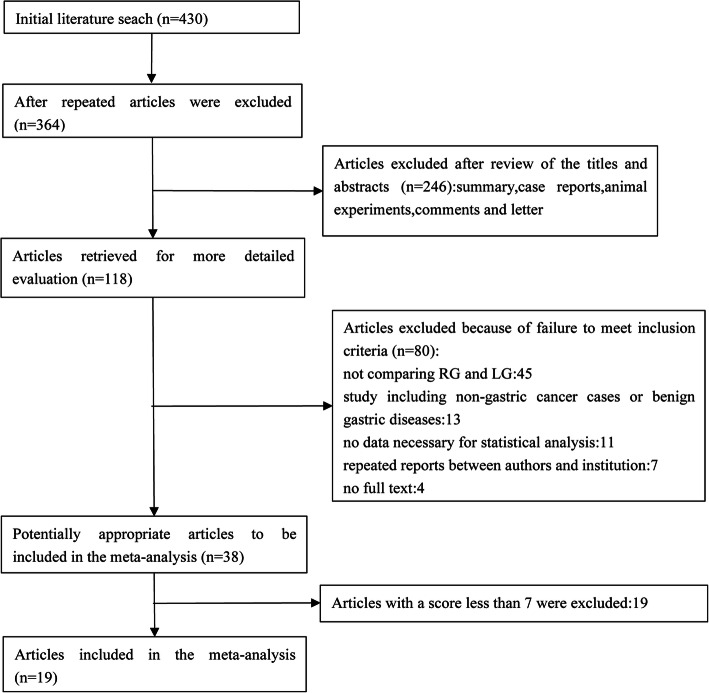
Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement was applied to perform the study. Pubmed, Cochrane Library, WanFang, China National Knowledge Infrastructure (CNKI), and VIP databases were comprehensively searched for studies published before May 2020 that compared RG with LG. Next, two independent reviewers conducted literature screening and data extraction. The quality of the literature was assessed using the Newcastle-Ottawa Scale (NOS), and the data analyzed using the Review Manager 5.3 software. Random effects or fixed effects models were applied according to heterogeneity.
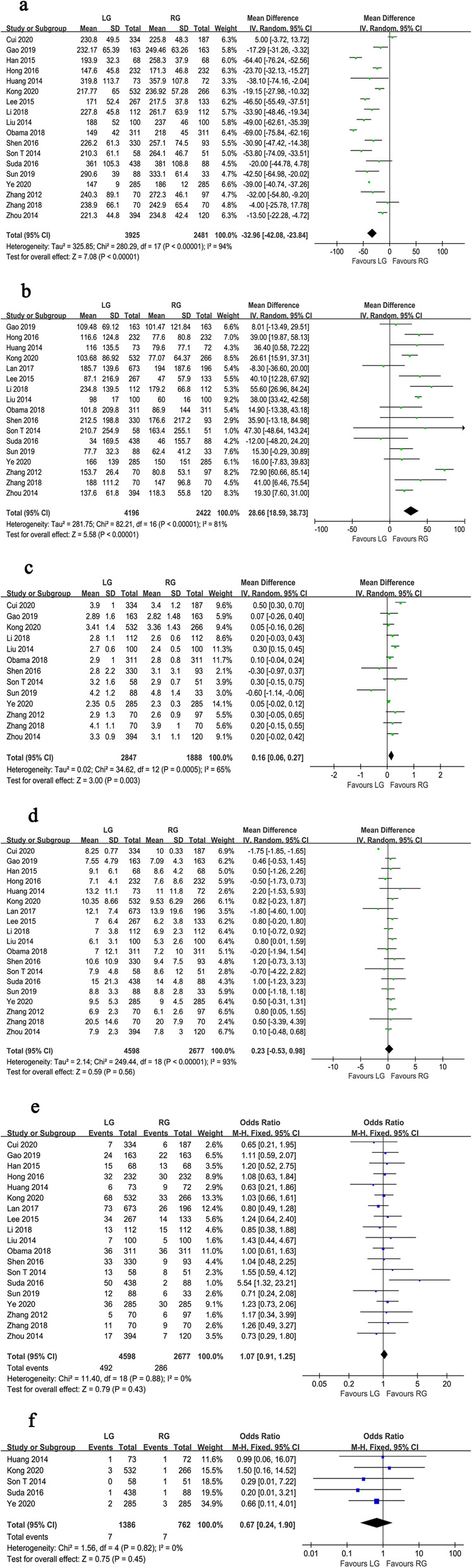
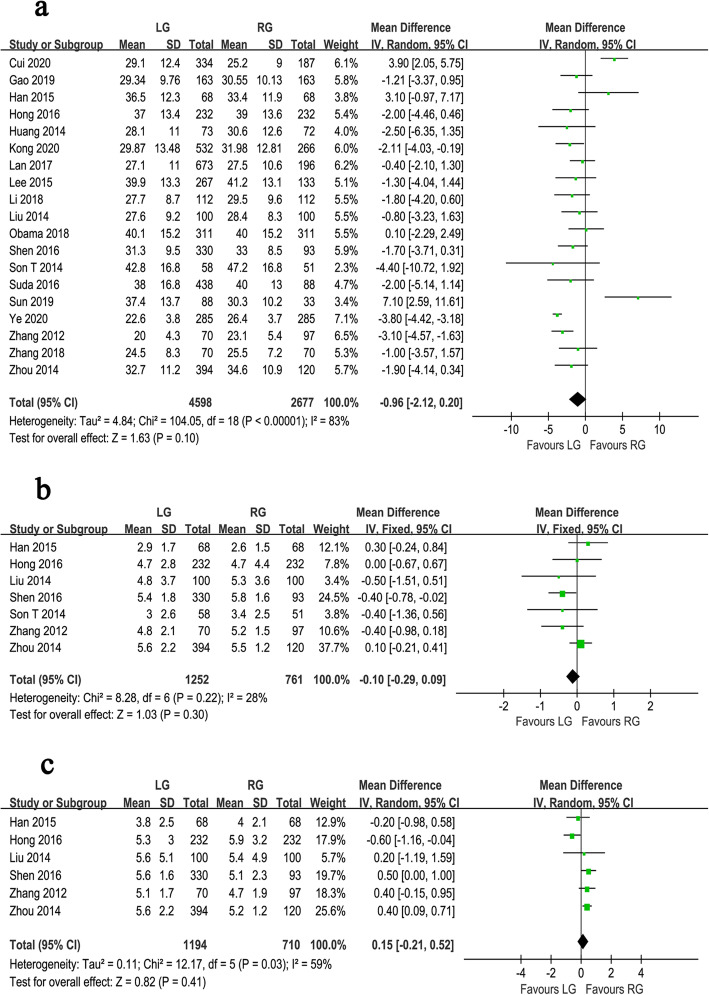
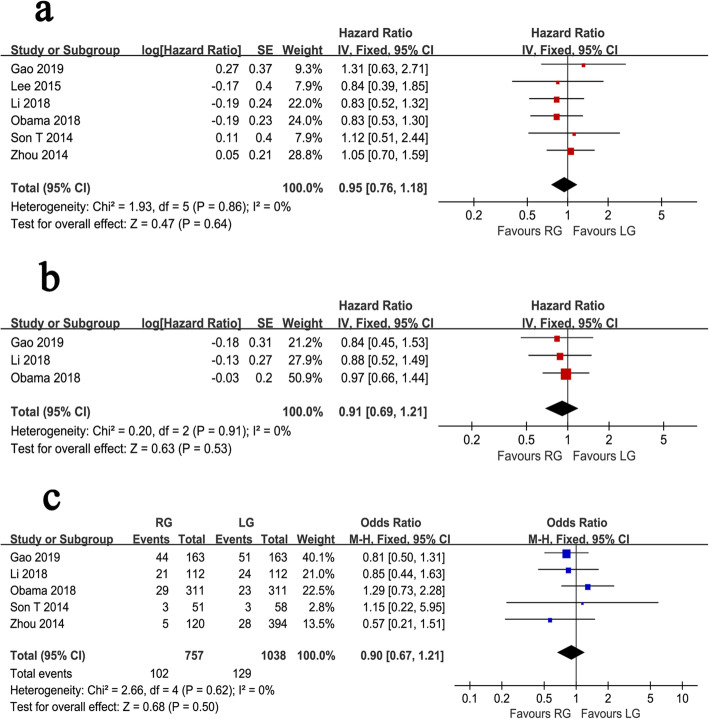
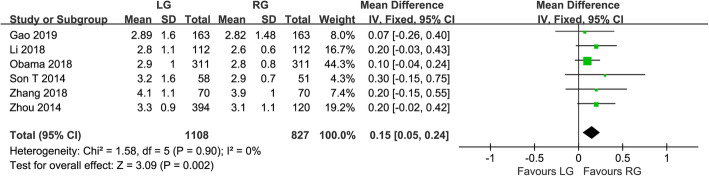
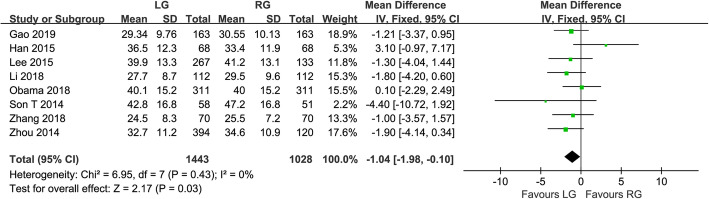
Results: A total of 19 studies including 7275 patients were included in the meta-analyses, of which 4598 patients were in the LG group and 2677 in the RG group. Compared with LG, RG was associated with longer operative time (WMD = -32.96, 95% CI -42.08 ~ -23.84, P < 0.001), less blood loss (WMD = 28.66, 95% CI 18.59 ~ 38.73, P < 0.001), and shorter time to first flatus (WMD = 0.16 95% CI 0.06 ~ 0.27, P = 0.003). There was no significant difference between RG and LG in terms of the hospital stay (WMD = 0.23, 95% CI -0.53 ~ 0.98, P = 0.560), overall postoperative complication (OR = 1.07, 95% CI 0.91 ~ 1.25, P = 0.430), mortality (OR = 0.67, 95% CI 0.24 ~ 1.90, P = 0.450), the number of harvested lymph nodes (WMD = -0.96, 95% CI -2.12 ~ 0.20, P = 0.100), proximal resection margin (WMD = -0.10, 95% CI -0.29 ~ 0.09, P = 0.300), and distal resection margin (WMD = 0.15, 95% CI -0.21 ~ 0.52, P = 0.410). No significant differences were found between the two treatments in overall survival (OS) (HR = 0.95, 95% CI 0.76 ~ 1.18, P = 0.640), recurrence-free survival (RFS) (HR = 0.91, 95% CI 0.69 ~ 1.21, P = 0.530), and recurrence rate (OR = 0.90, 95% CI 0.67 ~ 1.21, P = 0.500).
Conclusions: The results of this study suggested that RG is as acceptable as LG in terms of short-term and long-term outcomes. RG can be performed as effectively and safely as LG. Moreover, more randomized controlled trials comparing the two techniques with rigorous study designs are still essential to evaluate the value of the robotic surgery for gastric cancer.
Keywords: Gastrectomy; Gastric cancer; Laparoscopic; Meta-analysis; Robotic.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effectiveness and safety of robotic gastrectomy versus laparoscopic gastrectomy for gastric cancer: a meta-analysis of 12,401 gastric cancer patients.Updates Surg. 2022 Feb;74(1):267-281. doi: 10.1007/s13304-021-01176-3. Epub 2021 Oct 16. Updates Surg. 2022. PMID: 34655427
-
Robotic Versus Laparoscopic Gastrectomy for Gastric Cancer: A Mega Meta-Analysis.Front Surg. 2022 Jun 28;9:895976. doi: 10.3389/fsurg.2022.895976. eCollection 2022. Front Surg. 2022. PMID: 35836604 Free PMC article. Review.
-
Robotic versus Laparoscopic Gastrectomy for Gastric Carcinoma: a Meta-Analysis of Efficacy and Safety.Asian Pac J Cancer Prev. 2016;17(9):4327-4333. Asian Pac J Cancer Prev. 2016. PMID: 27797239
-
Comparative analysis of robotic gastrectomy and laparoscopic gastrectomy for gastric cancer in terms of their long-term oncological outcomes: a meta-analysis of 3410 gastric cancer patients.World J Surg Oncol. 2019 May 23;17(1):86. doi: 10.1186/s12957-019-1628-2. World J Surg Oncol. 2019. PMID: 31122260 Free PMC article.
-
Robotic versus laparoscopic gastrectomy for gastric cancer: a meta-analysis of short outcomes.Surg Oncol. 2012 Dec;21(4):274-80. doi: 10.1016/j.suronc.2012.05.004. Epub 2012 Jul 11. Surg Oncol. 2012. PMID: 22789391 Review.
Cited by
-
Efficacy and safety of robotic vs. laparoscopic gastrectomy for patients with gastric cancer: systematic review and meta-analysis.Int J Surg. 2024 Dec 1;110(12):8045-8056. doi: 10.1097/JS9.0000000000001826. Int J Surg. 2024. PMID: 38874467 Free PMC article.
-
Perioperative outcomes of robot-assisted versus laparoscopic distal gastrectomy for gastric cancer: a systematic review and meta-analysis of propensity score matching studies.J Robot Surg. 2024 Sep 4;18(1):333. doi: 10.1007/s11701-024-02038-x. J Robot Surg. 2024. PMID: 39231865
-
Benefits of minimally invasive surgery in the treatment of gastric cancer.World J Gastroenterol. 2022 Aug 14;28(30):4227-4230. doi: 10.3748/wjg.v28.i30.4227. World J Gastroenterol. 2022. PMID: 36157117 Free PMC article.
-
Postoperative outcomes in robotic gastric resection compared with laparoscopic gastric resection in gastric cancer: A meta-analysis and systemic review.Health Sci Rep. 2022 Aug 16;5(5):e746. doi: 10.1002/hsr2.746. eCollection 2022 Sep. Health Sci Rep. 2022. PMID: 35989947 Free PMC article. Review.
-
Different surgical methods of hysterectomy for the management of endometrial cancer: a systematic review and network meta-analysis.Front Oncol. 2025 Jan 15;14:1524991. doi: 10.3389/fonc.2024.1524991. eCollection 2024. Front Oncol. 2025. PMID: 39882446 Free PMC article.
References
-
- Josep T, Paulo MH, Lin S, Atsushi O, Manish AS, Karen C, Chunyan S, Haiyan W, Jennifer EW, Katherine K, et al. Pertuzumab plus trastuzumab and chemotherapy for HER2-positive metastatic gastric or gastro-oesophageal junction cancer (JACOB): final analysis of a double-blind, randomised, placebo-controlled phase 3 study. Lancet Oncol. 2018;19:1372–1384. doi: 10.1016/S1470-2045(18)30481-9. - DOI - PubMed
-
- Kitano S, Iso Y, Moriyama M, Sugimachi K. Laparoscopy-assisted Billroth I gastrectomy. Surgical Laparoscopy & Endoscopy. 1994;4:146–148. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
