

doi: 10.1016/j.cpsurg.2020.100823.
Epub 2020 May 15.
Small Bowel Neuroendocrine Tumors
Affiliations
- PMID: 33234227
- PMCID: PMC7722476
- DOI: 10.1016/j.cpsurg.2020.100823
Item in Clipboard
Small Bowel Neuroendocrine Tumors
Curr Probl Surg.
2020 Dec.
No abstract available
Figures

Proposed mechanism for development of SBNETs. Loss of heterozygosity at chromosome 18 occurs in more than 60% of SBNETs, suggesting it is an early event in tumorigenesis. More than 7% of SBNETs have mutations in CDKN1B, , , but recurring mutations are uncommon, while gains of chromosome 14 and 7 and losses of 3p, 11q, and 13 are common.

Age-adjusted yearly incidence of NETs from all sites. The incidence of NETs has increased 6.4-fold from 1973 to 2012. Data from the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) database.

Image demonstrating flushing in a patient’s face (left) and legs (right) due to carcinoid syndrome secondary to an SBNET. The patient is a young woman who initially presented with postprandial flushing, nausea, vomiting, tachycardia, and diarrhea. She was determined to have a mid-ileal neuroendocrine tumor and multiple hepatic metastases.

A) Primary SBNET with dilated proximal bowel (held in surgeon’s right hand) and multifocal lesions (each black suture designates a different primary tumor). B) Primary SBNET (blue arrow) and adjacent nodal metastasis (white arrow). C) Peritoneal metastasis from an SBNET (tip of forceps).

Synthesis and excretion of serotonin by neuroendocrine tumor cells. Serotonin is stored in secretory vesicles in the cell and then released into the blood, where it is stored in platelets. Serotonin is converted to 5-hydroxyindoleacetic acid (5-HIAA), which is excreted in the urine. Serotonin is thought to be responsible for the symptoms of carcinoid syndrome.

A) CT scan showing a primary SBNET (white arrow). The patient is a 67 year old woman who presented with abdominal pain, diarrhea, and flushing. She was determined to have an ileal NET with numerous hepatic metastases. She underwent laparotomy, small bowel resection, and enucleation and ablation of multiple (>30) liver lesions. B) Coronal CT scan with nodal metastases (white arrow) from the same patient. Nodal metastases can cause a local desmoplastic response, causing calcifications and fibrosis that result in a characteristic stellate pattern with spiculations on CT (not present here). C) CT scan from this patient demonstrating multiple hypodense liver metastases on the venous phase (C, arrows), which on arterial phase D) tend to be hypervascular and appear as enhancing masses.

Axial MRI of hepatic metastases (arrows) from an SBNET in the same patient shown in Fig. 6. Metastases appear hypointense on Tl-weighed MRI (A) and hyperintense on T2-weighted MRI (B). C) 68Ga-DOTATATE scan showing primary SBNET (blue arrow), nodal metastasis (red arrow), and liver metastases (white arrows) in the same patient.

A: Low (A) and high-power (B) images of hematoxylin and eosin (H&E) staining of SBNET demonstrating nested architecture and ovoid, centrally located “salt-and-pepper” nuclei. Images courtesy of Andrew Bellizzi, MD. C) Immunohistochemistry results for H&E, CDX2, PAX6, and ISL1 staining. Small bowel NETs stain positive for CDX2 and negative for PAX6, ISL1 (top panel). Pancreatic NETs stain negative for CDX2 and positive for PAX6 and ISL1 (bottom panel). Image reprinted with permission from Surgery, 156(6), Maxwell JE, Sherman SK, Stashek KM, O’Dorisio TM, Bellizzi AM, Howe JR, A practical method to determine the site of unknown primary in metastatic neuroendocrine tumors, 1359–1365, copyright (2014), with permission from Elsevier. D) Images comparing H&E (left panels) and corresponding Ki-67 (right panels) staining of a metastatic, grade 3 neuroendocrine tumor with well- and “less well”-differentiated components. Panels A and B demonstrate a lower power view. Panels C and D demonstrate a higher power image of the well-differentiated component with Ki-67 of 0.75%. Panels E and F demonstrate a higher power image of the “less well”-differentiated component with a Ki-67 of 35%. Reprinted with permission from Human Pathology, Bellizzi AM, Immunohistochemistry in the diagnosis and classification of neuroendocrine neoplasms: what can brown do for you?, copyright (2019) with permission from Elsevier.

A: Low (A) and high-power (B) images of hematoxylin and eosin (H&E) staining of SBNET demonstrating nested architecture and ovoid, centrally located “salt-and-pepper” nuclei. Images courtesy of Andrew Bellizzi, MD. C) Immunohistochemistry results for H&E, CDX2, PAX6, and ISL1 staining. Small bowel NETs stain positive for CDX2 and negative for PAX6, ISL1 (top panel). Pancreatic NETs stain negative for CDX2 and positive for PAX6 and ISL1 (bottom panel). Image reprinted with permission from Surgery, 156(6), Maxwell JE, Sherman SK, Stashek KM, O’Dorisio TM, Bellizzi AM, Howe JR, A practical method to determine the site of unknown primary in metastatic neuroendocrine tumors, 1359–1365, copyright (2014), with permission from Elsevier. D) Images comparing H&E (left panels) and corresponding Ki-67 (right panels) staining of a metastatic, grade 3 neuroendocrine tumor with well- and “less well”-differentiated components. Panels A and B demonstrate a lower power view. Panels C and D demonstrate a higher power image of the well-differentiated component with Ki-67 of 0.75%. Panels E and F demonstrate a higher power image of the “less well”-differentiated component with a Ki-67 of 35%. Reprinted with permission from Human Pathology, Bellizzi AM, Immunohistochemistry in the diagnosis and classification of neuroendocrine neoplasms: what can brown do for you?, copyright (2019) with permission from Elsevier.
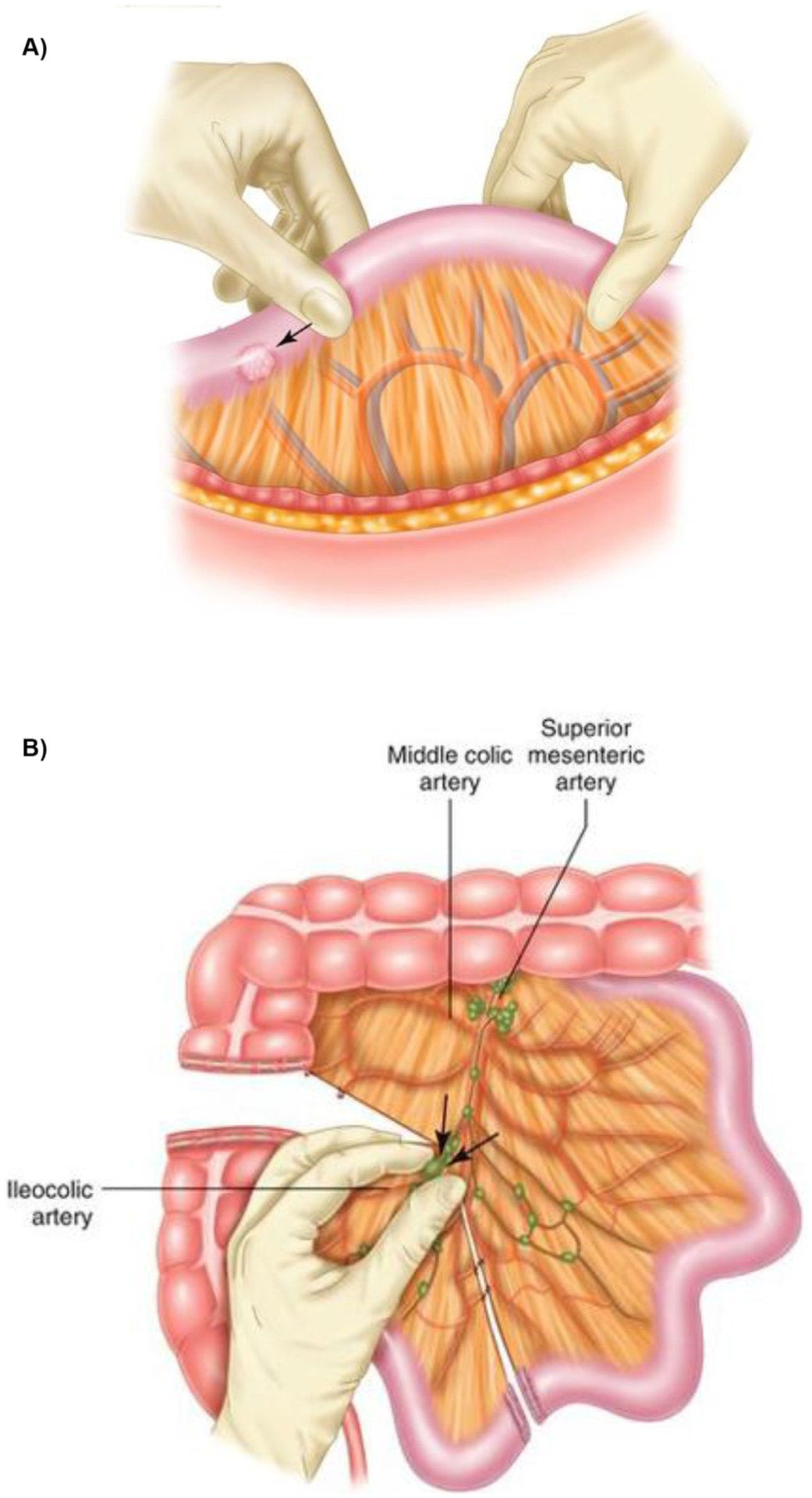
A) Palpation of the small bowel beginning from the ligament of Treitz. The small bowel should be carefully pulled through the thumb and forefinger to palpate for lesions. B) Dissection of the base of the ileocolic artery. The nodes are pulled away from the superior mesenteric artery and vein. Once the nodes are freed from the base of the mesentery, the proximal subsegmental vessels are doubly clamped and suture ligated. Reprinted by permission from Springer Nature: Small Bowel Resection and Lymphadenectomy for Jejunoileal Neuroendocrine Tumors by Howe, JR in Endocrine and Neuroendocrine Surgery, copyright 2017.

An algorithmic approach to the diagnosis and treatment of small bowel neuroendocrine tumors (NETs). BNP, brain natriuretic peptide; CAPTEM, capecitabine and temozolomide; CT, computed tomography; DTIC, dacarbazine; GaPET, gallium positron emission tomography; IFN, interferon; In-SRS, indium somatostatin receptor scintigraphy; IRI, irinotecan; LAR, long-acting repeatable; NEC, neuroendocrine carcinoma; OX, oxaliplatin; PRRT, peptide receptor radionuclide therapy; SSA, somatostatin analog; STZ, streptozocin; TMZ, temozolomide. Reprinted with permission from: Scott AT, Howe JR. Management of Small Bowel Neuroendocrine Tumors. J Oncol Pract. 2018;14(8):471–482. ©2018 American Society of Clinical Oncology. All rights reserved.
Similar articles
-
ENETS Consensus Guidelines for High-Grade Gastroenteropancreatic Neuroendocrine Tumors and Neuroendocrine Carcinomas.Neuroendocrinology. 2016;103(2):186-94. doi: 10.1159/000443172. Epub 2016 Jan 5. Neuroendocrinology. 2016. PMID: 26731334 No abstract available.
-
Management of Small Bowel Neuroendocrine Tumors.J Oncol Pract. 2018 Aug;14(8):471-482. doi: 10.1200/JOP.18.00135. J Oncol Pract. 2018. PMID: 30096273 Free PMC article. Review.
-
ENETS Consensus Guidelines for the management of patients with neuroendocrine neoplasms from the jejuno-ileum and the appendix including goblet cell carcinomas.Neuroendocrinology. 2012;95(2):135-56. doi: 10.1159/000335629. Epub 2012 Feb 15. Neuroendocrinology. 2012. PMID: 22262080 No abstract available.
-
[Progression of diagnosis and treatment in primary malignant small bowel tumor].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Jan 25;20(1):117-120. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 28105627 Review. Chinese.
-
ENETS Consensus Guidelines for the Standards of Care in Neuroendocrine Tumors: pre- and perioperative therapy in patients with neuroendocrine tumors.Neuroendocrinology. 2009;90(2):203-8. doi: 10.1159/000225949. Epub 2009 Aug 28. Neuroendocrinology. 2009. PMID: 19713712 No abstract available.
Cited by
-
Aggressiveness in Well-Differentiated Small Intestinal Neuroendocrine Tumors: A Rare Case and Narrative Literature Review.J Clin Med. 2025 Aug 18;14(16):5821. doi: 10.3390/jcm14165821. J Clin Med. 2025. PMID: 40869648 Free PMC article. Review.
-
Correlation between Neurotransmitters (Dopamine, Epinephrine, Norepinephrine, Serotonin), Prognostic Nutritional Index, Glasgow Prognostic Score, Systemic Inflammatory Response Markers, and TNM Staging in a Cohort of Colorectal Neuroendocrine Tumor Patients.Int J Mol Sci. 2024 Jun 26;25(13):6977. doi: 10.3390/ijms25136977. Int J Mol Sci. 2024. PMID: 39000088 Free PMC article.
-
Mechanistic role of miR-375 in regulating PDPK1 to promote progression of small bowel neuroendocrine tumors: a silico analysis.Discov Oncol. 2025 Jun 23;16(1):1187. doi: 10.1007/s12672-025-02872-x. Discov Oncol. 2025. PMID: 40549235 Free PMC article.
-
Small Bowel Neuroendocrine Tumors-10-Year Experience of the Ottawa Hospital (TOH).Curr Oncol. 2023 Aug 9;30(8):7508-7519. doi: 10.3390/curroncol30080544. Curr Oncol. 2023. PMID: 37623025 Free PMC article.
-
Endoscopic mucosal resection with double band ligation versus endoscopic submucosal dissection for small rectal neuroendocrine tumors.World J Gastrointest Surg. 2023 Mar 27;15(3):440-449. doi: 10.4240/wjgs.v15.i3.440. World J Gastrointest Surg. 2023. PMID: 37032804 Free PMC article.
References
-
- Langhans T Über einen Drüsenpolyp im ileum. Virchows Archiv. 1867;38(4):559–560.
-
- Lubarsch O Über den primären Krebs des Ileum nebst Bemerkungen über das gleichzeitige Vorkommen von Krebs und Tuberculose. Archiv für pathologische Anatomie und Physiologie und für klinische Medicin. 1888;111(2):280–317.
-
- Ransom W A case of primary carcinoma of the ileum. The Lancet. 1890;136(3507):1020–1023.
-
- Oberndorfer S Karzinoide tumoren des dunndarms. Frankfurt Z Path. 1907;1:426–432.
-
- Williams ED, Sandler M. The classification of carcinoid tumours. Lancet. 1963;1(7275):238–239. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
