

Computational modelling suggests that Barrett's oesophagus may be the precursor of all oesophageal adenocarcinomas
- PMID: 33234525
- PMCID: PMC8292551
- DOI: 10.1136/gutjnl-2020-321598
Computational modelling suggests that Barrett's oesophagus may be the precursor of all oesophageal adenocarcinomas
Abstract
Objective: Barrett's oesophagus (BE) is a known precursor to oesophageal adenocarcinoma (OAC) but current clinical data have not been consolidated to address whether BE is the origin of all incident OAC, which would reinforce evidence for BE screening efforts. We aimed to answer whether all expected prevalent BE, diagnosed and undiagnosed, could account for all incident OACs in the US cancer registry data.
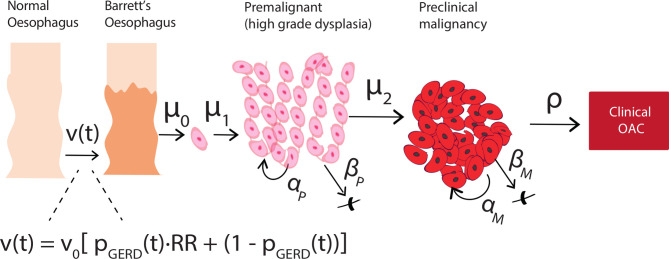
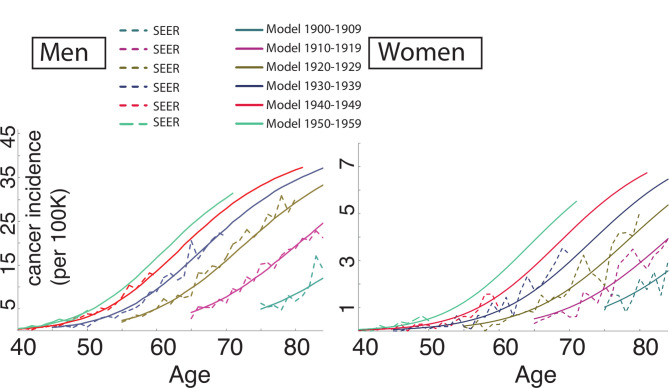
Design: We used a multiscale computational model of OAC that includes the evolutionary process from normal oesophagus through BE in individuals from the US population. The model was previously calibrated to fit Surveillance, Epidemiology and End Results cancer incidence curves. Here, we also utilised age-specific and sex-specific US census data for numbers at-risk. The primary outcome for model validation was the expected number of OAC cases for a given calendar year. Secondary outcomes included the comparisons of resulting model-predicted prevalence of BE and BE-to-OAC progression to the observed prevalence and progression rates.
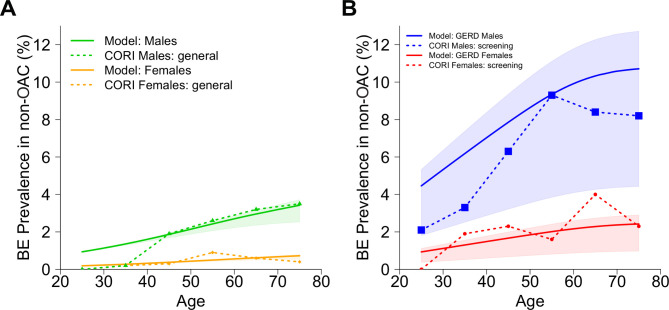
Results: The model estimated the total number of OAC cases from BE in 2010 was 9970 (95% CI: 9140 to 11 980), which recapitulates nearly all OAC cases from population data. The model simultaneously predicted 8%-9% BE prevalence in high-risk males age 45-55, and 0.1%-0.2% non-dysplastic BE-to-OAC annual progression in males, consistent with clinical studies.
Conclusion: There are likely few additional OAC cases arising in the US population outside those expected from individuals with BE. Effective screening of high-risk patients could capture the majority of population destined for OAC progression and potentially decrease mortality through early detection and curative removal of small (pre)cancers during surveillance.
Keywords: Barrett's carcinoma; Barrett's oesophagus; oesophageal cancer; pre-malignancy - gi tract; screening.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: KC, JHR and JMI declare no potential conflicts of interest. AC has founders shares and stock options in LucidDx, serves as a consultant to LucidDx, has sponsored research with LucidDx and has a royalty interest in patents licensed to LucidDx. He is also a consultant for Interpace Diagnostics and receives research support from C2 Therapeutics/Pentax.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources