

Unscheduled and out-of-hours care for people in their last year of life: a retrospective cohort analysis of national datasets
- PMID: 33234657
- PMCID: PMC7684800
- DOI: 10.1136/bmjopen-2020-041888
Unscheduled and out-of-hours care for people in their last year of life: a retrospective cohort analysis of national datasets
Abstract
Objectives: To analyse patterns of use and costs of unscheduled National Health Service (NHS) services for people in the last year of life.
Design: Retrospective cohort analysis of national datasets with application of standard UK costings.
Participants and setting: All people who died in Scotland in 2016 aged 18 or older (N=56 407).
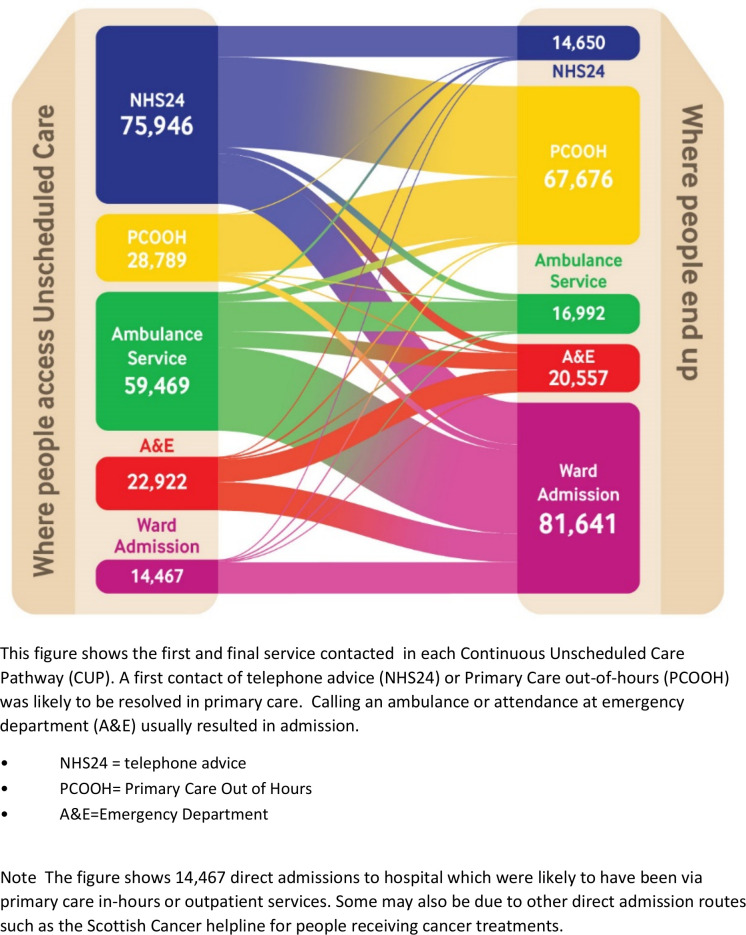
Main outcome measures: Frequency of use of the five unscheduled NHS services in the last 12 months of life by underlying cause of death, patient demographics, Continuous Unscheduled Pathways (CUPs) followed by patients during each care episode, total NHS and per-patient costs.
Results: 53 509 patients (94.9%) had at least one contact with an unscheduled care service during their last year of life (472 360 contacts), with 34.2% in the last month of life. By linking patient contacts during each episode of care, we identified 206 841 CUPs, with 133 980 (64.8%) starting out-of-hours. People with cancer were more likely to contact the NHS telephone advice line (63%) (χ2 (4)=1004, p<0.001) or primary care out-of-hours (62%) (χ2 (4)=1924,p<0.001) and have hospital admissions (88%) (χ2 (4)=2644, p<0.001). People with organ failure (79%) contacted the ambulance service most frequently (χ2 (4)=584, p<0.001). Demographic factors associated with more unscheduled care were older age, social deprivation, living in own home and dying of cancer. People dying with organ failure formed the largest group in the cohort and had the highest NHS costs as a group. The cost of providing services in the community was estimated at 3.9% of total unscheduled care costs despite handling most out-of-hours calls.
Conclusions: Over 90% of people used NHS unscheduled care in their last year of life. Different underlying causes of death and demographic factors impacted on initial access and subsequent pathways of care. Managing more unscheduled care episodes in the community has the potential to reduce hospital admissions and overall costs.
Keywords: accident & emergency medicine; adult palliative care; health services administration & management; primary care; public health; statistics & research methods.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: No support from any additional organisations for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- NHS Digital Hospital admitted patient care and adult critical care activity 2018-19, 2019. Available: https://files.digital.nhs.uk/F2/E70669/hosp-epis-stat-admi-summ-rep-2018...
-
- Institute of Medicine of the National Academies Dying in America: improving quality and honoring individual preferences near the end of life. Washington, DC: The National Academies Press, 2015. - PubMed
-
- World Health Assembly Strengthening of palliative care as a component of comprehensive care throughout the life course. resolution WHA67.19 adopted by the sixty-seventh World health assembly. Geneva: WHO, 2014.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources