

Factors associated with acute cardiac injury and their effects on mortality in patients with COVID-19
- PMID: 33235220
- PMCID: PMC7686361
- DOI: 10.1038/s41598-020-77172-1
Factors associated with acute cardiac injury and their effects on mortality in patients with COVID-19
Abstract
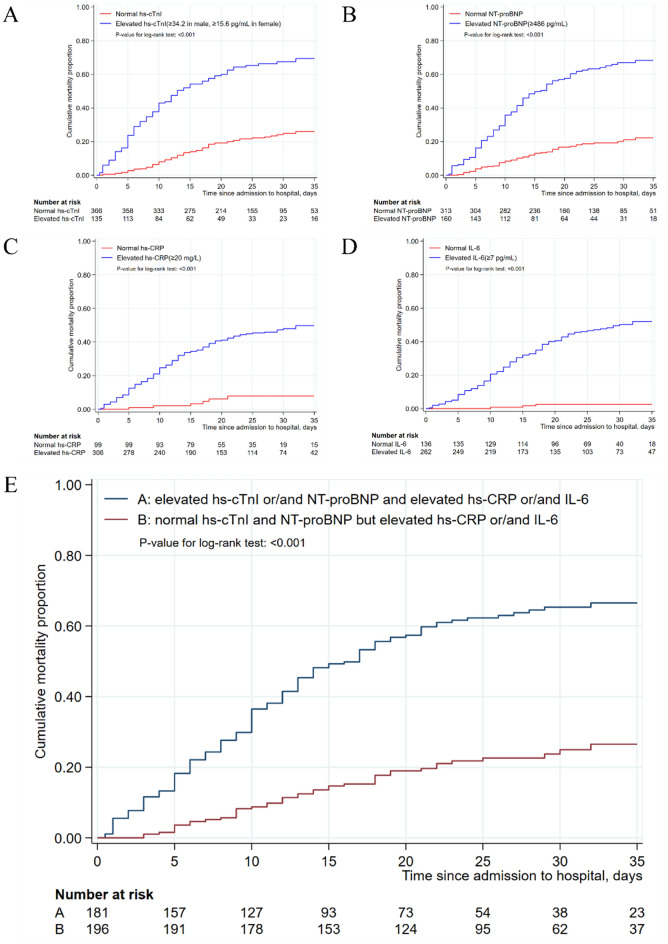
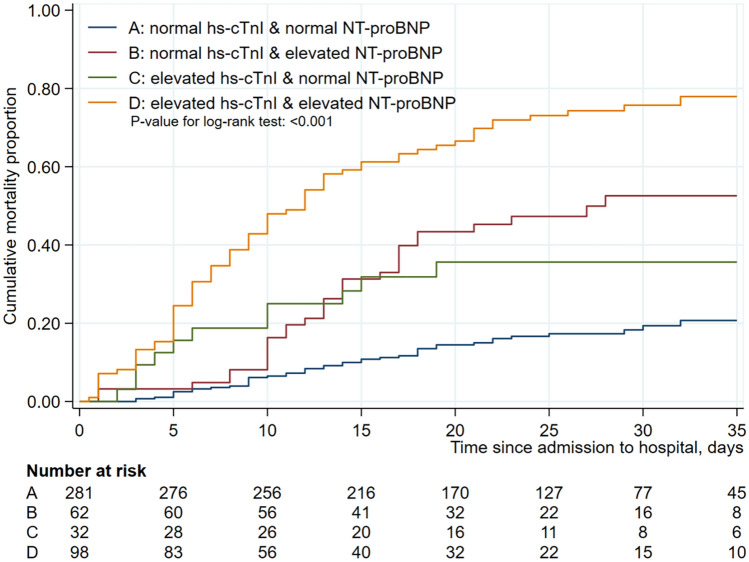
To determine the incidence of acute cardiac injury (ACI), the factors associated with ACI and the in-hospital mortality in patients with COVID-19, especially in severe patients. All consecutive in-patients with laboratory-confirmed COVID-19 from Tongji Hospital in Wuhan during February 1 and March 29, 2020 were included. The demographic, clinical characteristics, laboratory, radiological and treatment data were collected. Univariate and Firth logistic regression analyses were used to identify factors associated with ACI and in-hospital mortality, and Kaplan-Meier method was used to estimate cumulative in-hospital mortality. Among 1031 patients included, 215 (20.7%) had ACI and 501 (48.6%) were severe cases. Overall, 165 patients died; all were from the severe group, and 131 (79.39%) had ACI. ACI (OR = 2.34, P = 0.009), male gender (OR = 2.58, P = 0.001), oximeter oxygen saturation (OR = 0.90, P < 0.001), lactate dehydrogenase (OR = 3.26, P < 0.001), interleukin-6 (IL-6) (OR = 8.59, P < 0.001), high sensitivity C-reactive protein (hs-CRP) (OR = 3.29, P = 0.016), N-terminal pro brain natriuretic peptide (NT-proBNP) (OR = 2.94, P = 0.001) were independent risk factors for the in-hospital mortality in severe patients. The mortality was significantly increased among severe patients with elevated hs-CRP, IL-6, hs-cTnI, and/or NT-proBNP. Moreover, the mortality was significantly higher in patients with elevation of both hs-cTnI and NT proBNP than in those with elevation of either of them. ACI develops in a substantial proportion of patients with COVID-19, and is associated with the disease severity and in-hospital mortality. A combination of hs-cTnI and NT-proBNP is valuable in predicting the mortality.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. StatPearls. Treasure Island: StatPearls Publishing; 2020. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
