

The frequency of follicular T helper cells differs in acute and chronic neuroinflammation
- PMID: 33235306
- PMCID: PMC7686332
- DOI: 10.1038/s41598-020-77588-9
The frequency of follicular T helper cells differs in acute and chronic neuroinflammation
Abstract
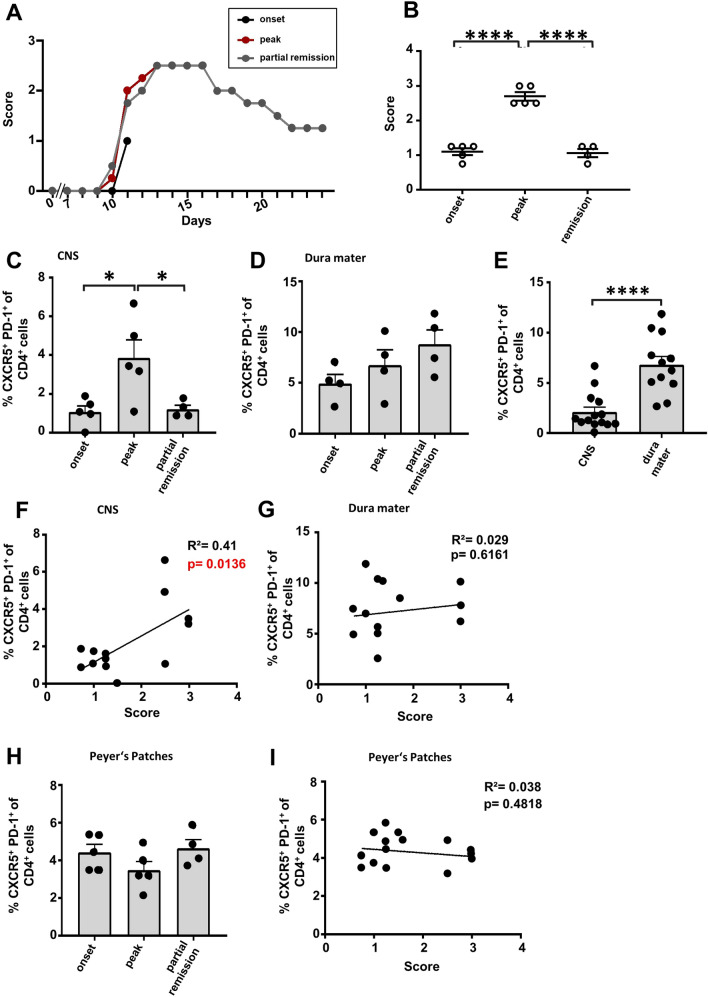
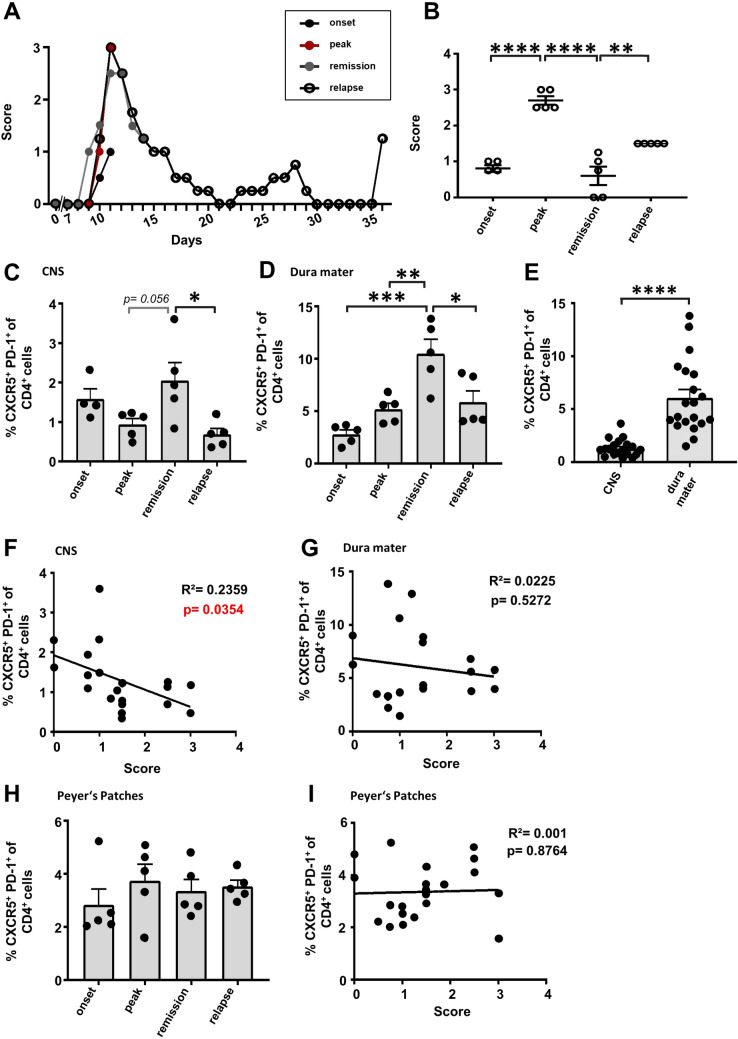
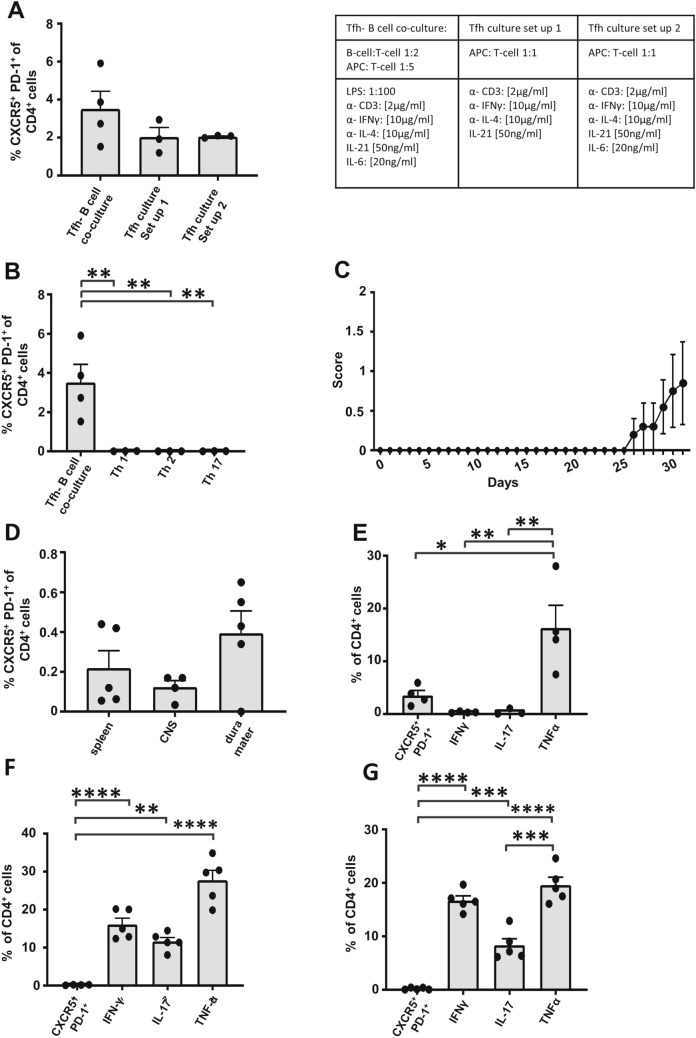
Beyond the major role of T cells in the pathogenesis of the autoimmune neuroinflammatory disorder multiple sclerosis (MS), recent studies have highlighted the impact of B cells on pathogenic inflammatory processes. Follicular T helper cells (Tfh) are essential for the promotion of B cell-driven immune responses. However, their role in MS and its murine model, experimental autoimmune encephalomyelitis (EAE), is poorly investigated. A first step to achieving a better understanding of the contribution of Tfh cells to the disease is the consideration of Tfh cell localization in relation to genetic background and EAE induction method. Here, we investigated the Tfh cell distribution during disease progression in disease relevant organs in three different EAE models. An increase of Tfh frequency in the central nervous system (CNS) was observed during peak of C57BL/6 J EAE, paralleling chronic disease activity, whereas in relapsing-remitting SJL EAE mice Tfh cell frequencies were increased during remission. Furthermore, transferred Tfh-skewed cells polarized in vitro induced mild clinical symptoms in B6.Rag1-/- mice. We identified significantly higher levels of Tfh cells in the dura mater than in the CNS both in C57BL/6 and in SJL/J mice. Overall, our study emphasizes diverse, non-static roles of Tfh cells during autoimmune neuroinflammation.
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
T Follicular Helper-Like Cells Are Involved in the Pathogenesis of Experimental Autoimmune Encephalomyelitis.Front Immunol. 2018 May 7;9:944. doi: 10.3389/fimmu.2018.00944. eCollection 2018. Front Immunol. 2018. PMID: 29867938 Free PMC article.
-
Methylprednisolone Modulates the Tfr/Tfh ratio in EAE-Induced Neuroinflammation through the PI3K/AKT/FoxO1 and PI3K/AKT/mTOR Signalling Pathways.Inflammation. 2025 Apr;48(2):950-962. doi: 10.1007/s10753-024-02099-y. Epub 2024 Jul 9. Inflammation. 2025. PMID: 38980500 Free PMC article.
-
Role of TFH Cells in Promoting T Helper 17-Induced Neuroinflammation.Front Immunol. 2018 Feb 27;9:382. doi: 10.3389/fimmu.2018.00382. eCollection 2018. Front Immunol. 2018. PMID: 29535739 Free PMC article.
-
Emerging Role of Follicular T Helper Cells in Multiple Sclerosis and Experimental Autoimmune Encephalomyelitis.Int J Mol Sci. 2018 Oct 19;19(10):3233. doi: 10.3390/ijms19103233. Int J Mol Sci. 2018. PMID: 30347676 Free PMC article. Review.
-
Emerging concepts in autoimmune encephalomyelitis beyond the CD4/T(H)1 paradigm.Ann Anat. 2010 Aug 20;192(4):179-93. doi: 10.1016/j.aanat.2010.06.006. Epub 2010 Jul 15. Ann Anat. 2010. PMID: 20692821 Review.
Cited by
-
T follicular helper cells contribute to pathophysiology in a model of neuromyelitis optica spectrum disorders.JCI Insight. 2023 Feb 22;8(4):e161003. doi: 10.1172/jci.insight.161003. JCI Insight. 2023. PMID: 36649074 Free PMC article.
-
Predicting Diagnostic Biomarkers Associated with Pyroptosis in Neuropathic Pain Based on Machine Learning and Experimental Validation.J Inflamm Res. 2024 Feb 20;17:1121-1145. doi: 10.2147/JIR.S445382. eCollection 2024. J Inflamm Res. 2024. PMID: 38406324 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
