

Multi-center nationwide comparison of seven serology assays reveals a SARS-CoV-2 non-responding seronegative subpopulation
- PMID: 33235985
- PMCID: PMC7676374
- DOI: 10.1016/j.eclinm.2020.100651
Multi-center nationwide comparison of seven serology assays reveals a SARS-CoV-2 non-responding seronegative subpopulation
Abstract
Background: An Israeli national taskforce performed a multi-center clinical and analytical validation of seven serology assays to determine their utility and limitations for SARS-CoV-2 diagnosis.
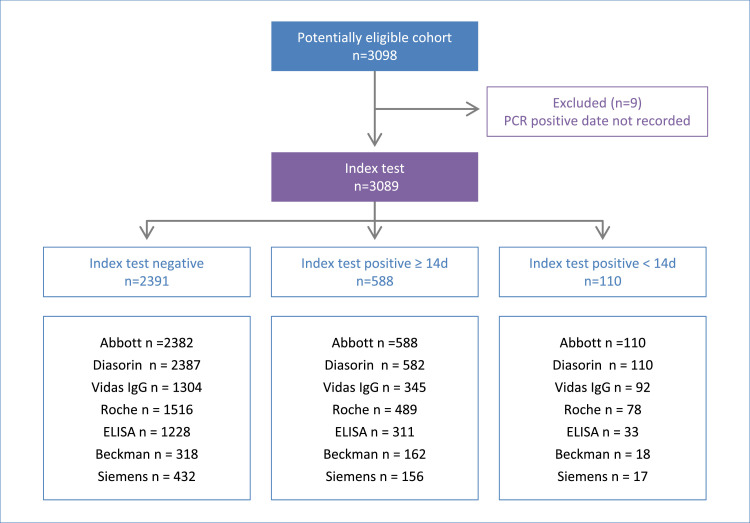
Methods: Serology assays from Roche, Abbott, Diasorin, BioMerieux, Beckman-Coulter, Siemens, and an in-house RBD ELISA were included. Negative samples from 2391 individuals representative of the Israeli population, and 698 SARS-CoV-2 PCR positive patients, collected between March and May 2020, were analyzed.
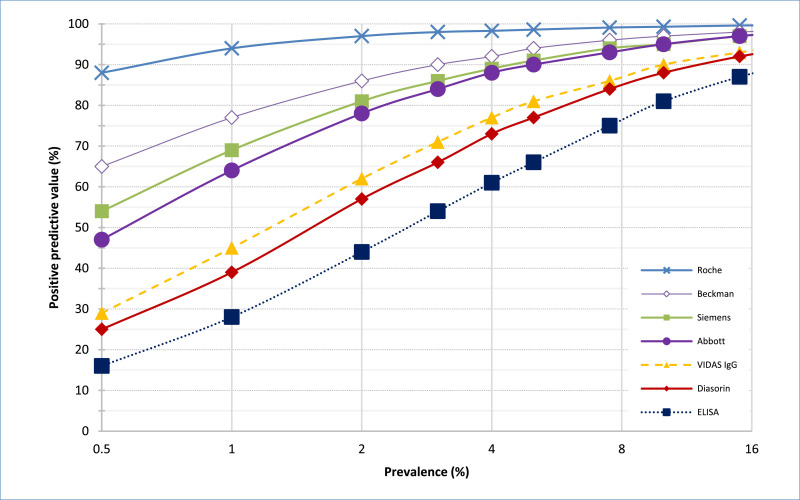
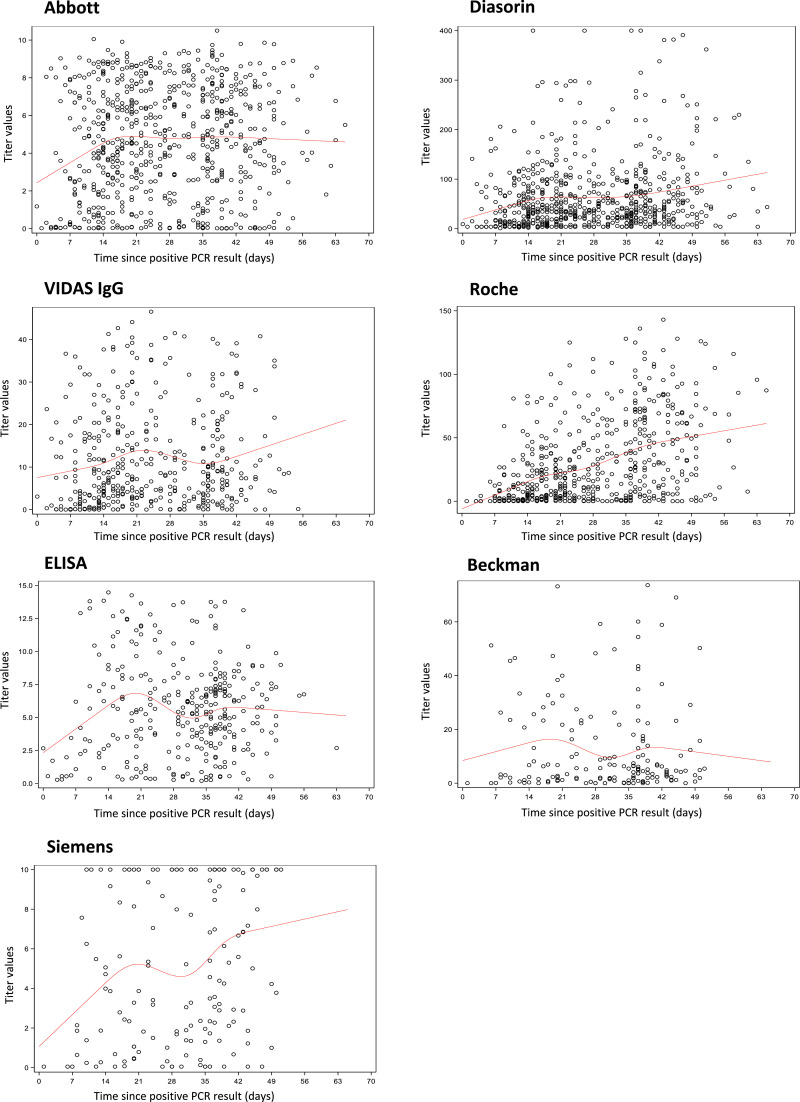
Findings: Immunoassays sensitivities between 81.5%-89.4% and specificities between 97.7%-100% resulted in a profound impact on the expected Positive Predictive Value (PPV) in low (<15%) prevalence scenarios. No meaningful increase was detected in the false positive rate in children compared to adults. A positive correlation between disease severity and antibody titers, and no decrease in antibody titers in the first 8 weeks after PCR positivity was observed. We identified a subgroup of symptomatic SARS-CoV-2 positive patients (~5% of patients), who remained seronegative across a wide range of antigens, isotypes, and technologies.
Interpretation: The commercially available automated immunoassays exhibit significant differences in performance and expected PPV in low prevalence scenarios. The low false-positivity rate in under 20's suggests that cross-reactive immunity from previous CoV strains is unlikely to explain the milder disease course in children. Finding no decrease in antibody titers in the first 8 weeks is in contrast to some reports of short half-life for SARS-CoV-2 antibodies. The ~5% who were seronegative non-responders, using multiple assays in a population-wide manner, represents the proportion of patients that may be at risk for re-infection.
Funding: Israel Ministry of Health.
Keywords: Antibodies; COVID-19; IgG; SARS-CoV-2; Serology; Seronegative subpopulation; Validation study.
© 2020 The Authors.
Conflict of interest statement
YL is supported by the Nehemia Rubin Excellence in Biomedical Research – The TELEM Program of Chaim Sheba Medical Center. All other authors have nothing to declare.
Figures
References
-
- Charlton C.L., Kanji J.N., Johal K., Bailey A., Plitt S.S., MacDonald C. Evaluation of six commercial mid to high volume antibody and six point of care lateral flow assays for detection of SARS-CoV-2 antibodies. J Clin Microbiol. 2020;58(10):e01361–20. doi: 10.1128/JCM.01361-20. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
