

Conversion from video-assisted thoracic surgery (VATS) to thoracotomy during major lung resection: how does it affect perioperative outcomes?
- PMID: 33236089
- PMCID: PMC8906703
- DOI: 10.1093/icvts/ivaa220
Conversion from video-assisted thoracic surgery (VATS) to thoracotomy during major lung resection: how does it affect perioperative outcomes?
Abstract
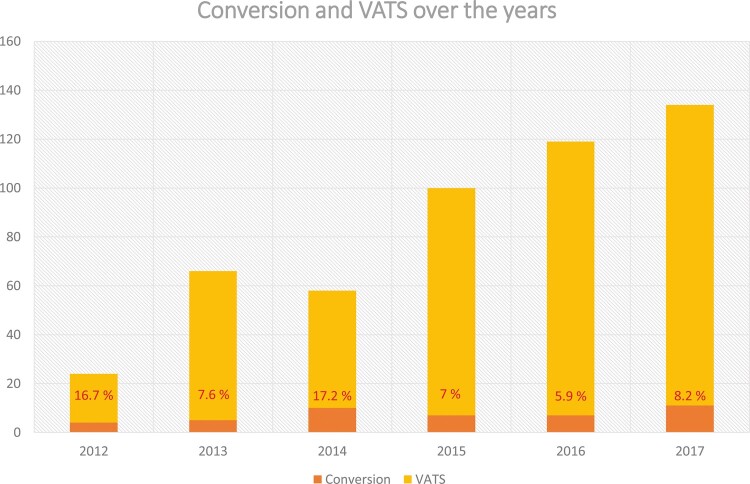
Objectives: Since video-assisted thoracic surgery (VATS) was first performed in the early 1990s, there have been many developments, and the conversion rate has decreased over the years. This article highlights the specific outcomes of patients undergoing conversion to thoracotomy despite initially scheduled VATS lung resection.
Methods: We retrospectively reviewed 501 patients who underwent thoracoscopic anatomic lung resection (i.e. lobectomy, segmentectomy or bilobectomy) between 1 January 2012 and 1 August 2017 at our institution. We explored the risk factors for surgical conversion and adverse events occurring in patients who underwent conversion to thoracotomy.
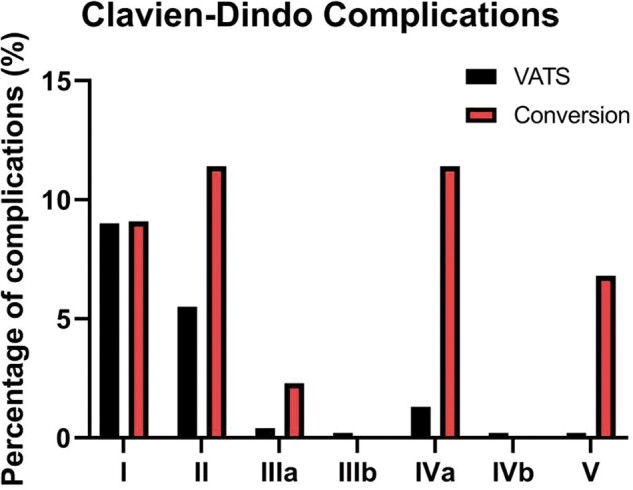
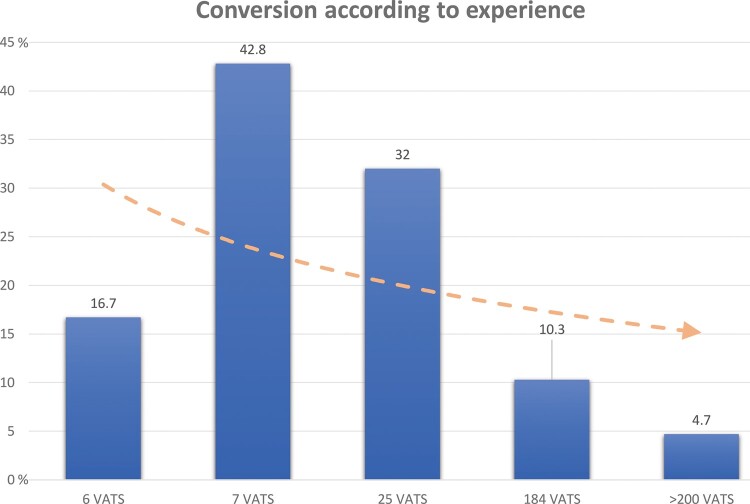
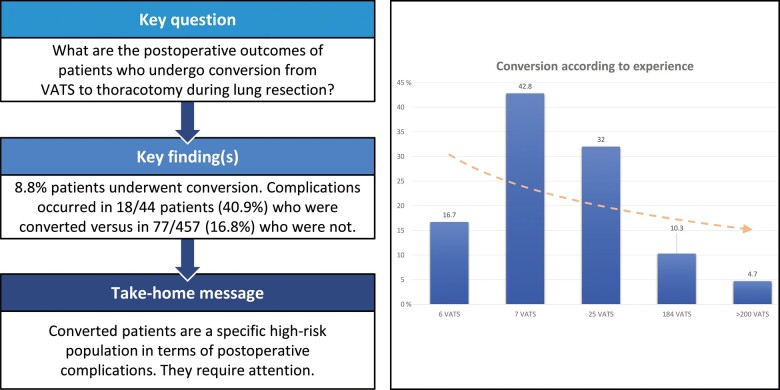
Results: A total of 44/501 patients underwent conversion during the procedure (global rate: 8.8%). The main reasons for conversion were (i) anatomical variation, adhesions or unexpected tumour extension (37%), followed by (ii) vascular causes (30%) and (iii) unexpected lymph node invasion (20%). The least common reason for conversion was technical failure (13%). We could not identify any specific risk factors for conversion. The global complication rate was significantly higher in converted patients (40.9%) than in complete VATS patients (16.8%) (P = 0.001). Postoperative atrial fibrillation was a major complication in converted patients (18.2%) [odds ratio (OR) 5.09, 95% confidence interval (CI) 1.80-13.27; P = 0.001]. Perioperative mortality was higher in the conversion group (6.8%) than in the VATS group (0.2%) (OR 33.3, 95% CI 3.4-328; P = 0.003).
Conclusions: Through the years, the global conversion rate has dramatically decreased to <10%. Nevertheless, patients who undergo conversion represent a high-risk population in terms of complications (40.9% vs 16.8%) and perioperative mortality (6.8% vs 0.2%).
Keywords: Conversion; Lung resection; Perioperative complications; Video-assisted thoracic surgery.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery. All rights reserved.
Figures
Similar articles
-
Comparative intention-to-treat analysis of the video-assisted thoracoscopic surgery approach to pulmonary segmentectomy for lung carcinoma‡.Interact Cardiovasc Thorac Surg. 2015 Sep;21(3):276-83. doi: 10.1093/icvts/ivv143. Epub 2015 Jun 10. Interact Cardiovasc Thorac Surg. 2015. PMID: 26063694
-
[Reasons for Conversion to Thoracotomy in 83 Cases during Video-assisted Thoracic Surgery Lobectomy: A Summary of 1,350 Consecutive Operations by A Single Surgical Team].Zhongguo Fei Ai Za Zhi. 2021 Jul 20;24(7):475-482. doi: 10.3779/j.issn.1009-3419.2021.101.21. Epub 2021 Jun 17. Zhongguo Fei Ai Za Zhi. 2021. PMID: 34134186 Free PMC article. Chinese.
-
Intraoperative conversion during video-assisted thoracoscopy does not constitute a treatment failure†.Eur J Cardiothorac Surg. 2019 Apr 1;55(4):660-665. doi: 10.1093/ejcts/ezy343. Eur J Cardiothorac Surg. 2019. PMID: 30325413
-
Does video-assisted thoracic surgery provide a safe alternative to conventional techniques in patients with limited pulmonary function who are otherwise suitable for lung resection?Interact Cardiovasc Thorac Surg. 2013 Jul;17(1):159-62. doi: 10.1093/icvts/ivt097. Epub 2013 Mar 26. Interact Cardiovasc Thorac Surg. 2013. PMID: 23532353 Free PMC article. Review.
-
Video-assisted thoracoscopic surgery versus muscle-sparing thoracotomy for non-small cell lung cancer: a systematic review and meta-analysis.BMC Surg. 2019 Oct 15;19(1):144. doi: 10.1186/s12893-019-0618-1. BMC Surg. 2019. PMID: 31615490 Free PMC article.
Cited by
-
Feasibility of video-assisted thoracoscopic surgery as a redo chest approach for lung resection in patients with a history of surgical procedures on the same side.J Thorac Dis. 2024 Oct 31;16(10):6879-6887. doi: 10.21037/jtd-24-216. Epub 2024 Oct 28. J Thorac Dis. 2024. PMID: 39552894 Free PMC article.
-
Clinical Efficacy of Thoracoscopic Surgery with the da Vinci Surgical System versus Video-Assisted Thoracoscopic Surgery for Lung Cancer.J Oncol. 2022 Jun 8;2022:5496872. doi: 10.1155/2022/5496872. eCollection 2022. J Oncol. 2022. PMID: 35720224 Free PMC article.
-
Effect of preoperative three-dimensional modeling on uniportal video-assisted thoracoscopic bronchial sleeve resection and early postoperative outcomes.Turk Gogus Kalp Damar Cerrahisi Derg. 2024 Apr 30;32(2):212-221. doi: 10.5606/tgkdc.dergisi.2024.26059. eCollection 2024 Apr. Turk Gogus Kalp Damar Cerrahisi Derg. 2024. PMID: 38933318 Free PMC article.
-
The Impact of Surgical Experience in VATS Lobectomy on Conversion and Patient Quality of Life: Results from a Comprehensive National Video-Assisted Thoracic Surgical Database.Cancers (Basel). 2023 Jan 8;15(2):410. doi: 10.3390/cancers15020410. Cancers (Basel). 2023. PMID: 36672359 Free PMC article.
-
Analysis of factors affecting intraoperative conversion from thoracoscopic radical resection of lung cancer to thoracotomy and intraoperative management experience.Pak J Med Sci. 2023 Sep-Oct;39(5):1389-1393. doi: 10.12669/pjms.39.5.7422. Pak J Med Sci. 2023. PMID: 37680827 Free PMC article.
References
-
- Hazelrigg SR, Nunchuck SK, LoCicero J. Video assisted thoracic surgery study group data. Ann Thorac Surg 1993;56:1039–43; discussion 1043–4. - PubMed
-
- Roviaro G, Rebuffat C, Varoli F, Vergani C, Mariani C, Maciocco M. Videoendoscopic pulmonary lobectomy for cancer. Surg Laparosc Endosc 1992;2:244–7. - PubMed
-
- Falcoz P-E, Puyraveau M, Thomas P-A, Decaluwe H, Hürtgen M, Petersen RH et al. Video-assisted thoracoscopic surgery versus open lobectomy for primary non-small-cell lung cancer: a propensity-matched analysis of outcome from the European Society of Thoracic Surgeon database. Eur J Cardiothorac Surg 2016;49:602–9. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
