

Reduction in acute kidney injury post cardiac surgery using balanced forced diuresis: a randomized, controlled trial
- PMID: 33236105
- PMCID: PMC8043764
- DOI: 10.1093/ejcts/ezaa395
Reduction in acute kidney injury post cardiac surgery using balanced forced diuresis: a randomized, controlled trial
Abstract
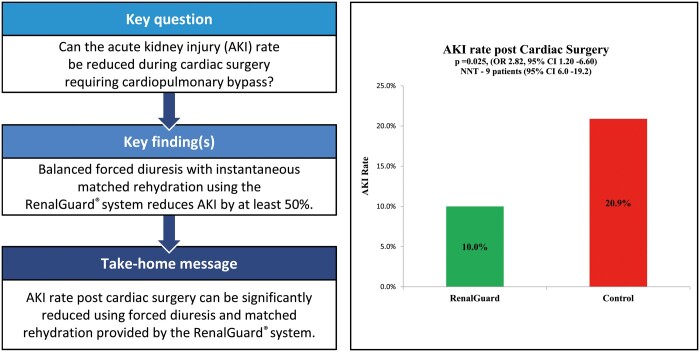
Objectives: Our goal was to investigate the efficacy of balanced forced diuresis in reducing the rate of acute kidney injury (AKI) in cardiac surgical patients requiring cardiopulmonary bypass (CPB), using the RenalGuard® (RG) system.
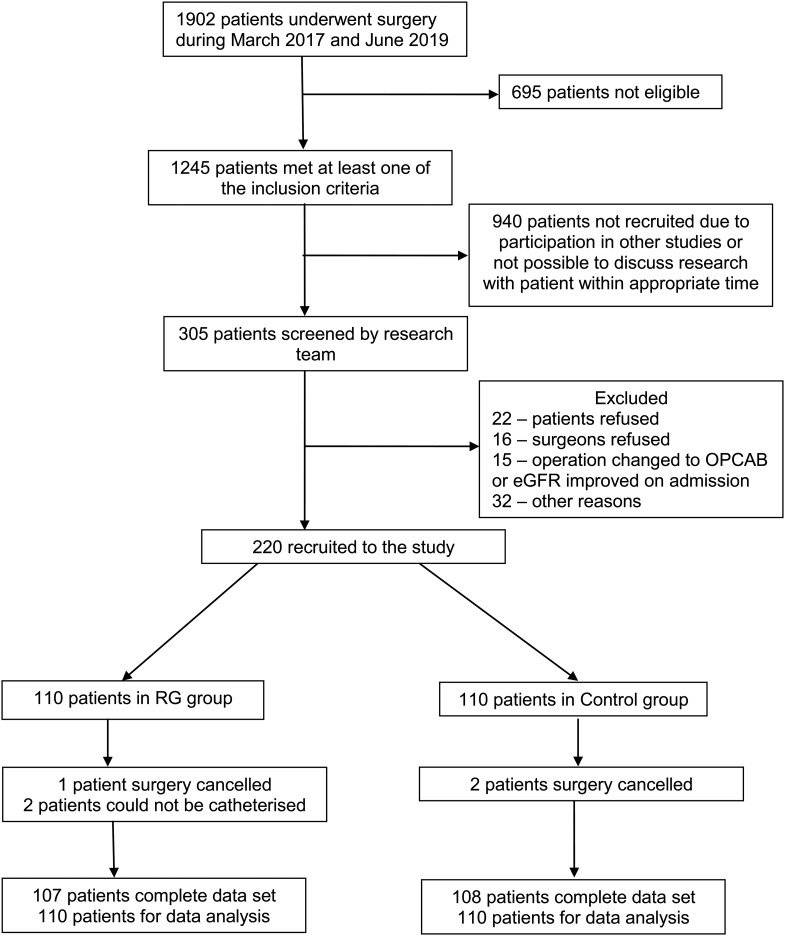
Methods: Patients at risk of developing AKI (history of diabetes and/or anaemia; estimated glomerular filtration rate 20-60 ml/min/1.73 m2; anticipated CPB time >120 min; log EuroSCORE > 5) were randomized to the RG system group (n = 110) or managed according to current practice (control = 110). The primary end point was the development of AKI within the first 3 postoperative days as defined by the RIFLE (Risk, Injury, Failure, Loss of kidney function, End-stage renal disease) criteria.
Results: There were no significant differences in preoperative and intraoperative characteristics between the 2 groups. Postoperative AKI rates were significantly lower in the RG system group compared to the control group [10% (11/110) vs 20.9% (23/110); P = 0.025]. This effect persisted even after controlling for a number of potential confounders (odds ratio 2.82, 95% confidence interval 1.20-6.60; P = 0.017) when assessed by binary logistic regression analysis. The mean volumes of urine produced during surgery and within the first 24 h postoperatively were significantly higher in the RG system group (P < 0.001). There were no significant differences in the incidence of blood transfusions, atrial fibrillation and infections and in the median duration of intensive care unit stays between the groups. The number needed to treat with the RG system to prevent AKI was 9 patients (95% confidence interval 6.0-19.2).
Conclusions: In patients at risk for AKI who had cardiac surgery with CPB, the RS RG system significantly reduced the incidence of AKI and can be used safely and reproducibly. Larger studies are required to confirm cost benefits.
Clinical trial registration number: NCT02974946.
Keywords: Acute kidney injury; Cardiac surgery; RenalGuard®; system.
© The Author(s) 2020. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
Similar articles
-
Balanced forced-diuresis compared to control as a reno-protective approach in cardiac surgery: secondary outcome of a randomized controlled trial, assessment of neutrophil gelatinase-associated lipocalin levels.J Cardiothorac Surg. 2021 Aug 24;16(1):240. doi: 10.1186/s13019-021-01620-w. J Cardiothorac Surg. 2021. PMID: 34429137 Free PMC article. Clinical Trial.
-
Balanced forced-diuresis as a renal protective approach in cardiac surgery: Secondary outcomes of electrolyte changes.J Card Surg. 2021 Nov;36(11):4125-4131. doi: 10.1111/jocs.15925. Epub 2021 Aug 19. J Card Surg. 2021. PMID: 34414606 Free PMC article. Clinical Trial.
-
Risk factor for acute kidney injury in patients with chronic kidney disease receiving valve surgery with cardiopulmonary bypass.Asian J Surg. 2021 Jan;44(1):229-234. doi: 10.1016/j.asjsur.2020.05.024. Epub 2020 Jul 2. Asian J Surg. 2021. PMID: 32624399
-
Goal-directed perfusion for reducing acute kidney injury in cardiac surgery: A systematic review and meta-analysis.Perfusion. 2023 Apr;38(3):591-599. doi: 10.1177/02676591211073783. Epub 2022 Feb 6. Perfusion. 2023. PMID: 35125028
-
Cardiac surgery-associated acute kidney injury.Blood Purif. 2014;37 Suppl 2:34-50. doi: 10.1159/000361062. Epub 2014 Jul 31. Blood Purif. 2014. PMID: 25196567 Review.
Cited by
-
Future insights of pharmacological prevention for AKI post cardiopulmonary bypass surgery (based on PK/PD approach).Front Pharmacol. 2022 Sep 22;13:975641. doi: 10.3389/fphar.2022.975641. eCollection 2022. Front Pharmacol. 2022. PMID: 36210841 Free PMC article. Review.
-
Diuretic treatment using the RenalGuard® system in patients hospitalized due to acute decompensated heart failure and characterization of the profile of patients with good and poor response to treatment - preliminary study.Cardiol J. 2025;32(1):43-52. doi: 10.5603/cj.102386. Epub 2024 Nov 21. Cardiol J. 2025. PMID: 39570006 Free PMC article.
-
Acute Kidney Injury Prevention Following Cardiac Catheterization: The Ins and Outs of Management.Kidney Med. 2024 Jul 11;6(8):100865. doi: 10.1016/j.xkme.2024.100865. eCollection 2024 Aug. Kidney Med. 2024. PMID: 39157195 Free PMC article. No abstract available.
-
Effect of Ascorbic Acid on Cardiac Surgery-Associated Acute Kidney Injury Incidence.Thorac Cardiovasc Surg. 2022 Oct;70(7):566-574. doi: 10.1055/s-0042-1744262. Epub 2022 May 28. Thorac Cardiovasc Surg. 2022. PMID: 35643076 Free PMC article. Clinical Trial.
-
Complications of Cardiopulmonary Bypass From an Anesthesia Perspective: A Clinical Review.HCA Healthc J Med. 2023 Feb 28;4(1):13-21. doi: 10.36518/2689-0216.1525. eCollection 2023. HCA Healthc J Med. 2023. PMID: 37426558 Free PMC article. Review.
References
-
- Wang Y, Bellomo R.. Cardiac surgery-associated acute kidney injury: risk factors, pathophysiology and treatment. Nat Rev Nephrol 2017;13:697–711. - PubMed
-
- Joannidis M, Druml W, Forni LG, Groeneveld ABJ, Honore PM, Hoste E. et al. Prevention of acute kidney injury and protection of renal function in the ICU: update 2017: expert opinion of the Working Group on Prevention, AKI section, European Society of Intensive Care Medicine. Intensive Care Med 2017;43:730–49. - PMC - PubMed
-
- Luckraz H, Gravenor MB, George R, Taylor S, Williams A, Ashraf S. et al. Long and short-term outcomes in patients requiring continuous renal replacement therapy post cardiopulmonary-bypass. Eur J Cardiothorac Surg 2005;27:906–9. - PubMed
