

MR Imaging of the Perihepatic Space
- PMID: 33236541
- PMCID: PMC8005346
- DOI: 10.3348/kjr.2019.0774
MR Imaging of the Perihepatic Space
Abstract
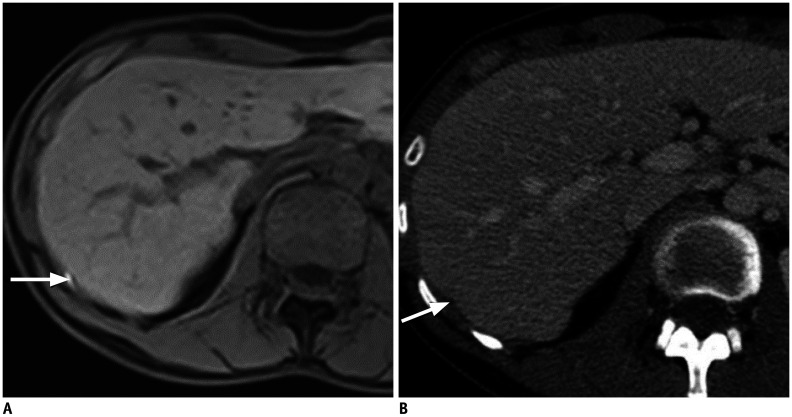
The perihepatic space is frequently involved in a spectrum of diseases, including intrahepatic lesions extending to the liver capsule and disease conditions involving adjacent organs extending to the perihepatic space or spreading thanks to the communication from intraperitoneal or extraperitoneal sites through the hepatic ligaments. Lesions resulting from the dissemination of peritoneal processes may also affect the perihepatic space. Here we discuss how to assess the perihepatic origin of a lesion and describe the magnetic resonance imaging (MRI) features of normal structures and fluids that may be abnormally located in the perihepatic space. We then review and illustrate the MRI findings present in cases of perihepatic infectious, tumor-related, and miscellaneous conditions. Finally, we highlight the value of MRI over computed tomography.
Keywords: Computed tomography; Liver; Magnetic resonance imaging; Peritoneum.
Copyright © 2021 The Korean Society of Radiology.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures













References
-
- Kim S, Kim TU, Lee JW, Lee TH, Lee SH, Jeon TY, et al. The perihepatic space: comprehensive anatomy and CT features of pathologic conditions. Radiographics. 2007;27:129–143. - PubMed
-
- Tirkes T, Sandrasegaran K, Patel AA, Hollar MA, Tejada JG, Tann M, et al. Peritoneal and retroperitoneal anatomy and its relevance for cross-sectional imaging. Radiographics. 2012;32:437–451. - PubMed
-
- DeMeo JH, Fulcher AS, Austin RF., Jr Anatomic CT demonstration of the peritoneal spaces, ligaments, and mesenteries: normal and pathologic processes. Radiographics. 1995;15:755–770. - PubMed
-
- Oh SN, Rha SE, Byun JY, Kim JY, Song KY, Park CH. Chilaiditi syndrome caused by Fitz-Hugh-Curtis syndrome: multidetector CT findings. Abdom Imaging. 2006;31:45–47. - PubMed
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
