

Progress in Imaging the Human Torso at the Ultrahigh Fields of 7 and 10.5 T
- PMID: 33237019
- PMCID: PMC7713902
- DOI: 10.1016/j.mric.2020.10.001
Progress in Imaging the Human Torso at the Ultrahigh Fields of 7 and 10.5 T
Abstract
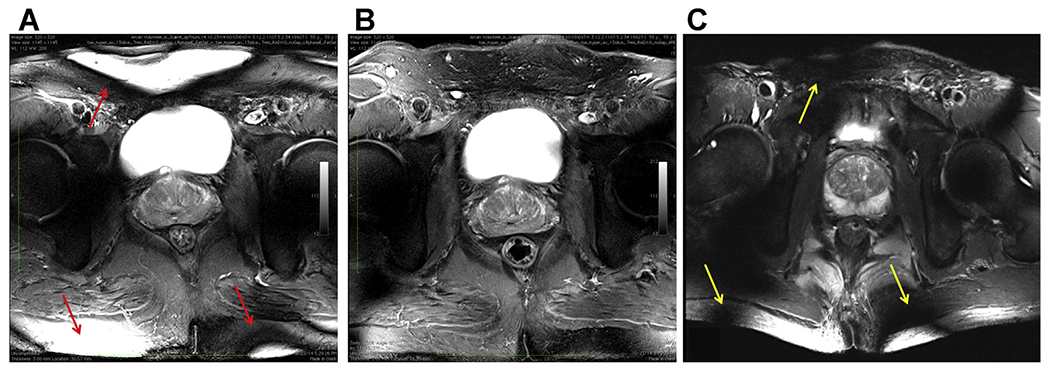
Especially after the launch of 7 T, the ultrahigh magnetic field (UHF) imaging community achieved critically important strides in our understanding of the physics of radiofrequency interactions in the human body, which in turn has led to solutions for the challenges posed by such UHFs. As a result, the originally obtained poor image quality has progressed to the high-quality and high-resolution images obtained at 7 T and now at 10.5 T in the human torso. Despite these tremendous advances, work still remains to further improve the image quality and fully capitalize on the potential advantages UHF has to offer.
Keywords: 10.5 T; 7 T; Imaging; Parallel transmit; Torso; Ultrahigh fields.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure The work reported in this article coming from the Center for Magnetic Resonance Research (CMRR), University of Minnesota was supported by NIH grants NIBIBP41 EB015894, NIBIB P41 EB027061, and NIH S10 RR029672.
Figures
References
-
- Vaughan JT, Snyder C, DelaBarre L, et al. in Proc Intl Soc Mag Reson Med Vol. 16 213 (Seattle, Washington, 2006).
-
- Umutlu L, Ladd ME, Forsting M, et al. 7 Tesla MR imaging: opportunities and challenges. Rofo 2014;186:121–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
