

Pharmacogenetics at Scale: An Analysis of the UK Biobank
- PMID: 33237584
- PMCID: PMC8144239
- DOI: 10.1002/cpt.2122
Pharmacogenetics at Scale: An Analysis of the UK Biobank
Abstract
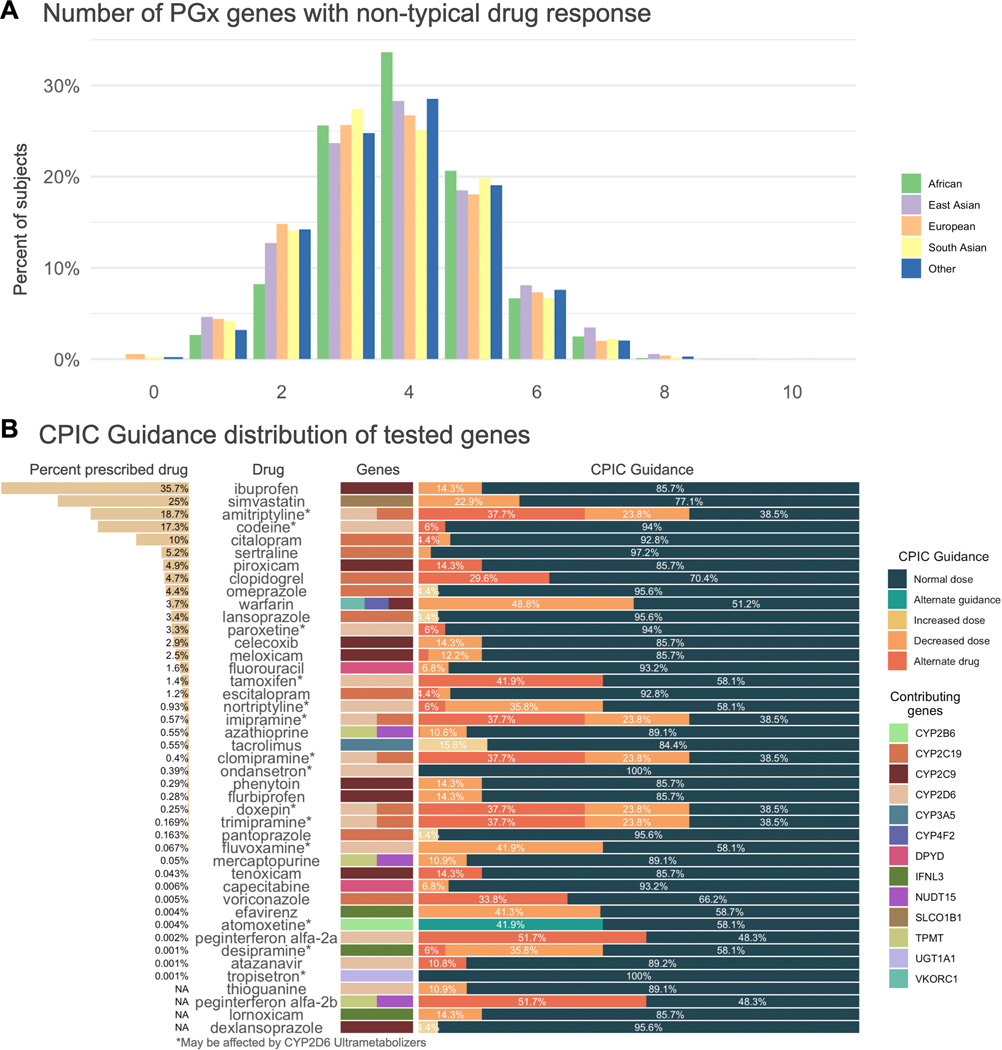
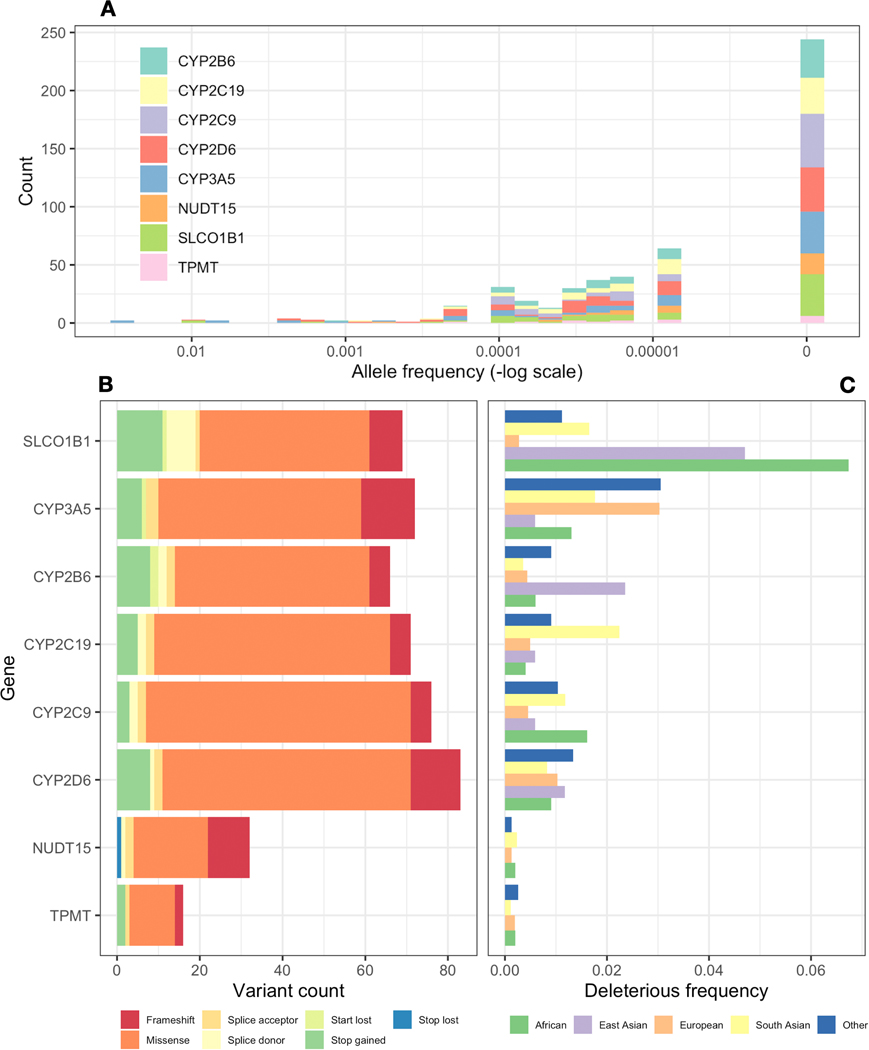
Pharmacogenetics (PGx) studies the influence of genetic variation on drug response. Clinically actionable associations inform guidelines created by the Clinical Pharmacogenetics Implementation Consortium (CPIC), but the broad impact of genetic variation on entire populations is not well understood. We analyzed PGx allele and phenotype frequencies for 487,409 participants in the UK Biobank, the largest PGx study to date. For 14 CPIC pharmacogenes known to influence human drug response, we find that 99.5% of individuals may have an atypical response to at least 1 drug; on average they may have an atypical response to 10.3 drugs. Nearly 24% of participants have been prescribed a drug for which they are predicted to have an atypical response. Non-European populations carry a greater frequency of variants that are predicted to be functionally deleterious; many of these are not captured by current PGx allele definitions. Strategies for detecting and interpreting rare variation will be critical for enabling broad application of pharmacogenetics.
© 2020 The Author Clinical Pharmacology & Therapeutics © 2020 American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
Conflict of Interests
R.B.A. is a stockholder in
Figures
References
-
- 2016 NAMCS Summary Web Tables. At <https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2016_namcs_web_tables.pdf>
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
