

Decline in SARS-CoV-2 Antibodies After Mild Infection Among Frontline Health Care Personnel in a Multistate Hospital Network - 12 States, April-August 2020
- PMID: 33237893
- PMCID: PMC7727600
- DOI: 10.15585/mmwr.mm6947a2
Decline in SARS-CoV-2 Antibodies After Mild Infection Among Frontline Health Care Personnel in a Multistate Hospital Network - 12 States, April-August 2020
Abstract
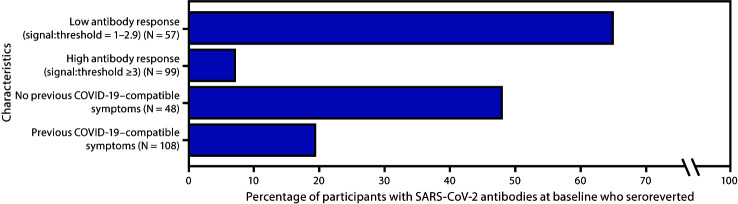
Most persons infected with SARS-CoV-2, the virus that causes coronavirus disease 2019 (COVID-19), develop virus-specific antibodies within several weeks, but antibody titers might decline over time. Understanding the timeline of antibody decline is important for interpreting SARS-CoV-2 serology results. Serum specimens were collected from a convenience sample of frontline health care personnel at 13 hospitals and tested for antibodies to SARS-CoV-2 during April 3-June 19, 2020, and again approximately 60 days later to assess this timeline. The percentage of participants who experienced seroreversion, defined as an antibody signal-to-threshold ratio >1.0 at baseline and <1.0 at the follow-up visit, was assessed. Overall, 194 (6.0%) of 3,248 participants had detectable antibodies to SARS-CoV-2 at baseline (1). Upon repeat testing approximately 60 days later (range = 50-91 days), 146 (93.6%) of 156 participants experienced a decline in antibody response indicated by a lower signal-to-threshold ratio at the follow-up visit, compared with the baseline visit, and 44 (28.2%) experienced seroreversion. Participants with higher initial antibody responses were more likely to have antibodies detected at the follow-up test than were those who had a lower initial antibody response. Whether decay in these antibodies increases risk for reinfection and disease remains unanswered. However, these results suggest that serology testing at a single time point is likely to underestimate the number of persons with previous SARS-CoV-2 infection, and a negative serologic test result might not reliably exclude prior infection.
Conflict of interest statement
All authors have completed and submitted the International Committee of Medical Journal Editors form for disclosure of potential conflicts of interest. Christopher J. Lindsell reports grants from National Institutes of Health, grants from Department of Defense, Marcus Foundation, Endpoint Health, Entegrion, bioMerieux, and Bioscape Digital, outside the submitted work. Daniel J. Henning reports personal fees from CytoVale and grants from Baxter, outside the submitted work. Akram Khan reports grants from United Therapeutics, Actelion Pharmaceuticals, Regeneron, and Reata Pharmaceuticals, outside the submitted work. Samuel M. Brown reports grants from National Institutes of Health, Department of Defense, Intermountain Research and Medical Foundation, and Janssen; consulting fees paid to his employer from Faron and Sedana, all outside the submitted work. Ithan D. Peltan reports grants from the National Institutes of Health and, outside the submitted work, grants from Asahi Kasei Pharma, Immunexpress Inc., Janssen Pharmaceuticals, and Regeneron. Carlos Grijalva reports other from Pfizer, other from Merck, other from Sanofi-Pasteur, grants from Campbell Alliance, the National Institutes of Health, the Food and Drug Administration, the Agency for Health Care Research and Quality, outside the submitted work. Todd W. Rice reports consulting work for Cumberland Pharmaceuticals, Inc, outside the submitted work. H. Keipp Talbot has served on a data safety and monitoring board for Seqirus. Natasha Halasa receives grant support from Quidel and Sanofi, donation of vaccines and hemagglutination inhibition/microneutralization titers performed by Sanofi, and speaker fees by an educational grant supported by Genentech, outside the submitted work. No other potential conflicts of interest were disclosed.
Figures
References
-
- Self WH, Tenforde MW, Stubblefield WB, et al. ; CDC COVID-19 Response Team; IVY Network. Seroprevalence of SARS-CoV-2 among frontline health care personnel in a multistate hospital network—13 academic medical centers, April–June 2020. MMWR Morb Mortal Wkly Rep 2020;69:1221–6. 10.15585/mmwr.mm6935e2 - DOI - PMC - PubMed
