

Characterisation of 22445 patients attending UK emergency departments with suspected COVID-19 infection: Observational cohort study
- PMID: 33237907
- PMCID: PMC7688143
- DOI: 10.1371/journal.pone.0240206
Characterisation of 22445 patients attending UK emergency departments with suspected COVID-19 infection: Observational cohort study
Abstract
Background: Hospital emergency departments play a crucial role in the initial assessment and management of suspected COVID-19 infection. This needs to be guided by studies of people presenting with suspected COVID-19, including those admitted and discharged, and those who do not ultimately have COVID-19 confirmed. We aimed to characterise patients attending emergency departments with suspected COVID-19, including subgroups based on sex, ethnicity and COVID-19 test results.
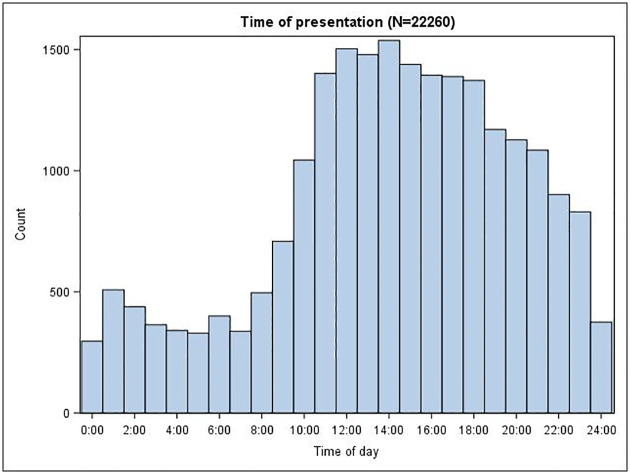
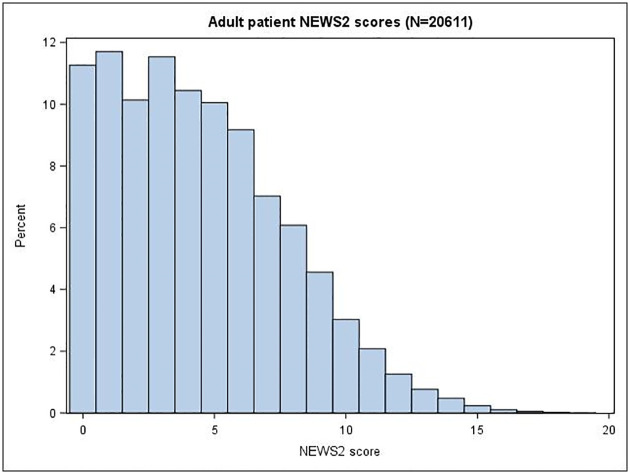
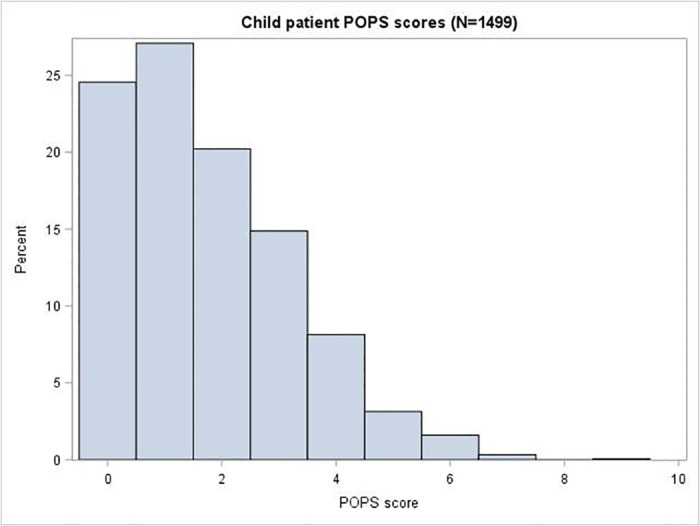
Methods and findings: We undertook a mixed prospective and retrospective observational cohort study in 70 emergency departments across the United Kingdom (UK). We collected presenting data from 22445 people attending with suspected COVID-19 between 26 March 2020 and 28 May 2020. Outcomes were admission to hospital, COVID-19 result, organ support (respiratory, cardiovascular or renal), and death, by record review at 30 days. Mean age was 58.4 years, 11200 (50.4%) were female and 11034 (49.6%) male. Adults (age >16 years) were acutely unwell (median NEWS2 score of 4), frequently had limited performance status (46.9%) and had high rates of admission (67.1%), COVID-19 positivity (31.2%), organ support (9.8%) and death (15.5%). Children had much lower rates of admission (27.4%), COVID-19 positivity (1.2%), organ support (1.4%) and death (0.3%). Similar numbers of men and women presented to the ED, but men were more likely to be admitted (72.9% v 61.4%), require organ support (12.2% v 7.7%) and die (18.2% v 13.0%). Black or Asian adults tended to be younger than White adults (median age 54, 50 and 67 years), were less likely to have impaired performance status (43.1%, 26.8% and 51.6%), be admitted to hospital (60.8%, 57.3%, 69.6%) or die (11.6%, 11.2%, 16.4%), but were more likely to require organ support (15.9%, 14.3%, 8.9%) or have a positive COVID-19 test (40.8%, 42.1%, 30.0%). Adults admitted with suspected and confirmed COVID-19 had similar age, performance status and comorbidities (except chronic lung disease) to those who did not have COVID-19 confirmed, but were much more likely to need organ support (22.2% v 8.9%) or die (32.1% v 15.5%).
Conclusions: Important differences exist between patient groups presenting to the emergency department with suspected COVID-19. Adults and children differ markedly and require different approaches to emergency triage. Admission and adverse outcome rates among adults suggest that policies to avoid unnecessary ED attendance achieved their aim. Subsequent COVID-19 confirmation confers a worse prognosis and greater need for organ support.
Registration: ISRCTN registry, ISRCTN56149622, http://www.isrctn.com/ISRCTN28342533.
Conflict of interest statement
All authors declare grant funding to their employing institutions from the National Institute for Health Research (NIHR), as outlined under financial disclosure information. SG is Deputy Director of the NIHR Health Technology Assessment (HTA) Programme, which funded the study, and chairs the NIHR HTA commissioning committee. These competing interests do not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- World Health Organisation. Clinical care of severe acute respiratory infections—Tool kit. https://www.who.int/publications-detail/clinical-care-of-severe-acute-re... (accessed 28/04/2020)
-
- International Federation for Emergency Medicine. Global Response to COVID-19 for Emergency Healthcare Systems and Providers: From the IFEM Task Force on ED Crowding and Access Block. https://www.ifem.cc/coronavirus-2019-information/ (accessed 15/06/2020)
-
- NHS. Clinical guide for the management of emergency department patients during the coronavirus pandemic. 17 March 2020 Version 1 https://www.england.nhs.uk/coronavirus/secondary-care/other-resources/sp... (accessed 15/06/2020)
-
- National Institute for Health and Care Excellence. COVID-19 rapid guideline: managing suspected or confirmed pneumonia in adults in the community. Published: 3 April 2020. www.nice.org.uk/guidance/ng165 (accessed 28/04/2020) - PubMed
-
- American College of Emergency Physicians. Guide to Coronavirus Disease (COVID-19) https://www.acep.org/corona/covid-19-field-guide/cover-page/
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
