

The impact of hypertension on chronic kidney disease and end-stage renal disease is greater in men than women: a systematic review and meta-analysis
- PMID: 33238919
- PMCID: PMC7687699
- DOI: 10.1186/s12882-020-02151-7
The impact of hypertension on chronic kidney disease and end-stage renal disease is greater in men than women: a systematic review and meta-analysis
Erratum in
-
Correction to: The impact of hypertension on chronic kidney disease and end-stage renal disease is greater in men than women: a systematic review and meta-analysis.BMC Nephrol. 2020 Dec 21;21(1):545. doi: 10.1186/s12882-020-02199-5. BMC Nephrol. 2020. PMID: 33349232 Free PMC article. No abstract available.
Abstract
Background: Hypertension (HTN) is an established risk factor for chronic kidney disease (CKD) and end-stage renal disease (ESRD). Whether sex differences in the effect of HTN on CKD and ESRD incidence exist remains unclear. This systematic review and meta-analysis was conducted to evaluate the relative impact of HTN on CKD and ESRD risk in women compared with men.
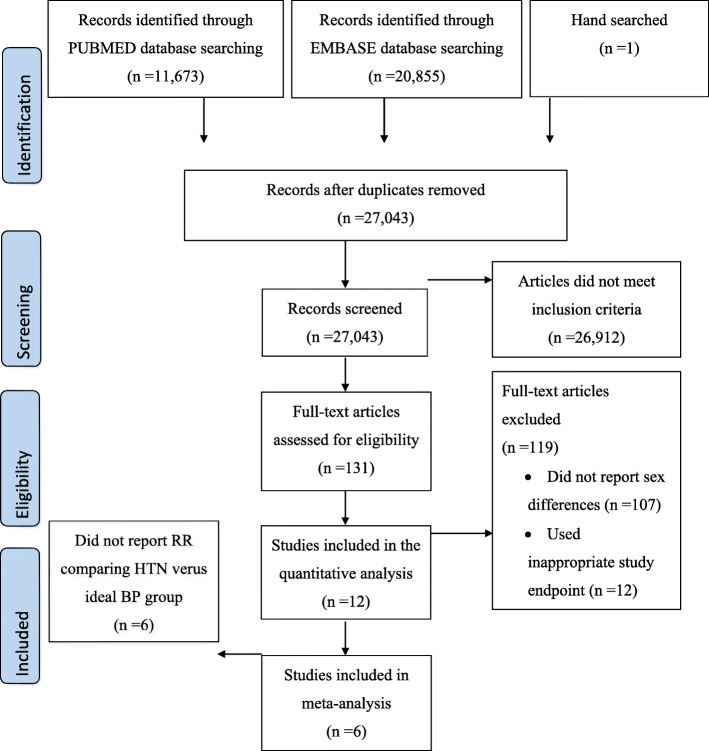
Methods: We systematically searched Embase and PubMed for cohort studies until 24 July 2020. Studies were selected if they reported a sex-specific association between systolic blood pressure (SBP) and CKD or ESRD. Random effects meta-analyses with inverse variance weighting were used to pool sex-specific relative risks (RRs) and the women-to-men ratio of RRs (the RRR) for incident CKD and ESRD.
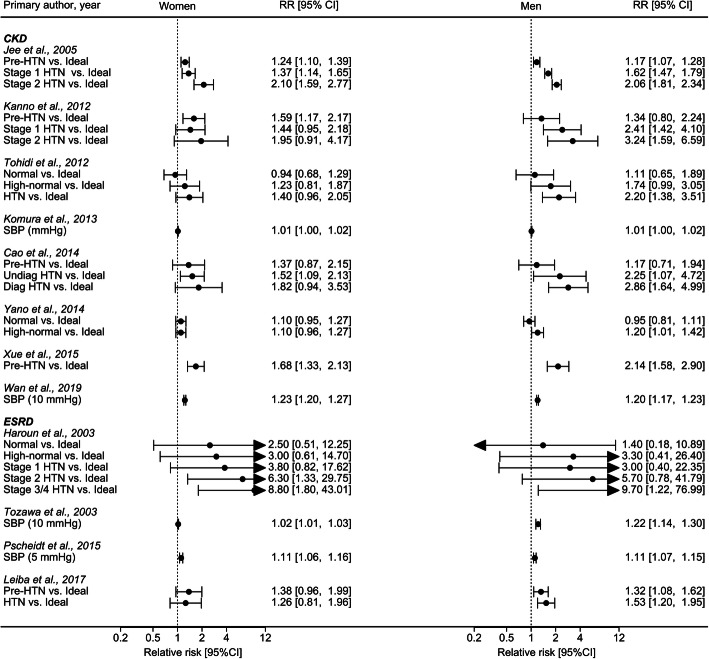
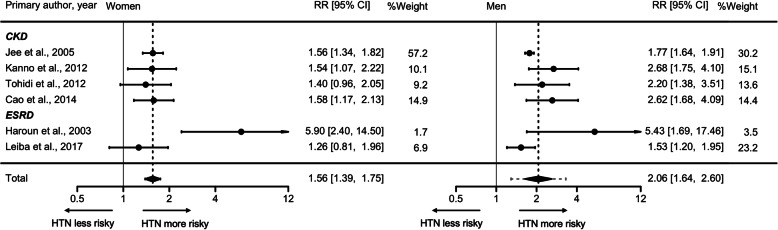
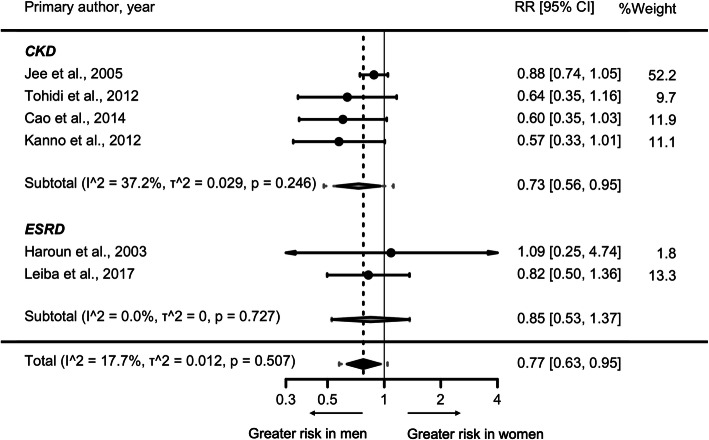
Results: Data from six cohorts, including 2,382,712 individuals and 6856 incident CKD events, and 833 ESRD events, were included in the meta-analysis. The RR for incident CKD or ESRD associated with HTN (SBP ≥140 mmHg) versus ideal BP (SBP < 120 mmHg) was 1.56 (95% CI, 1.39-1.75) in women and 2.06 (95% CI, 1.64-2.60) in men. The RR for incident CKD or ESRD was 23% lower in women than in men RRR 0.77 [95% CI, 0.63-0.95] with no significant heterogeneity between studies (p-value for Q test = 0.507, I2 = 17.7%).
Conclusion: HTN confers about a fifth lower excess risk of incident CKD or ESRD in women than men. Sex differences in onset, duration, and severity of some risk factors, such as albuminuria, diabetes, cardiovascular disease, obesity, and socioeconomic status, may explain part of the excess risk in men. Another explanation could be that women might be under-diagnosed and less likely to initiate dialysis. Future studies are needed to demonstrate the mechanisms responsible for the observed sex difference.
Conflict of interest statement
M. Woodward is supported by a National Health and Medical Research Council fellowship (APP1080206) and Program Grant (APP1149987) and does consultancy for Amgen and Kyowa Hakko Kirin outside the submitted work.
Figures
References
-
- GBD 2017 DALYs and HALE Collaborators Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1859–1922. doi: 10.1016/S0140-6736(18)32335-3. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
