

Benefit of dosimetry distribution for patients with multiple brain metastases from non-small cell lung cancer by a Cyberknife stereotactic radiosurgery (SRS) system
- PMID: 33238967
- PMCID: PMC7687698
- DOI: 10.1186/s12885-020-07624-4
Benefit of dosimetry distribution for patients with multiple brain metastases from non-small cell lung cancer by a Cyberknife stereotactic radiosurgery (SRS) system
Abstract
Background: In order to obtain a high dose conformal index of tumor and steep dose fall-off in healthy tissues for brain metastasis stereotactic radiosurgery (SRS), the aim of this study was to investigate SRS planning optimization by comparing one multiple-lesions plan (MLP) with multiple single-lesion plans (SLPs) for patients with multiple brain metastases using the Cyberknife (CK) system.
Methods: Fifty non-small cell lung cancer (NSCLC) patients (28 males and 22 females) with 2-4 brain metastases, inter-tumour distances less than 3 cm, were retrospectively replanned with the original prescription dose (12-32 Gy) in the original fractions (1-3). Two different clinical CK SRS plans (SLPs and MLP) were generated for the same patients with the same collimator and prescription isodose line (62-68%) by the CK Multiplan System. Both SLPs and MLP were able to achieve > 95% PTV volume covered prescription dose and met the Timmerman 2011 organs at risk (brainstem, optic nerve and pituitary) constraints.
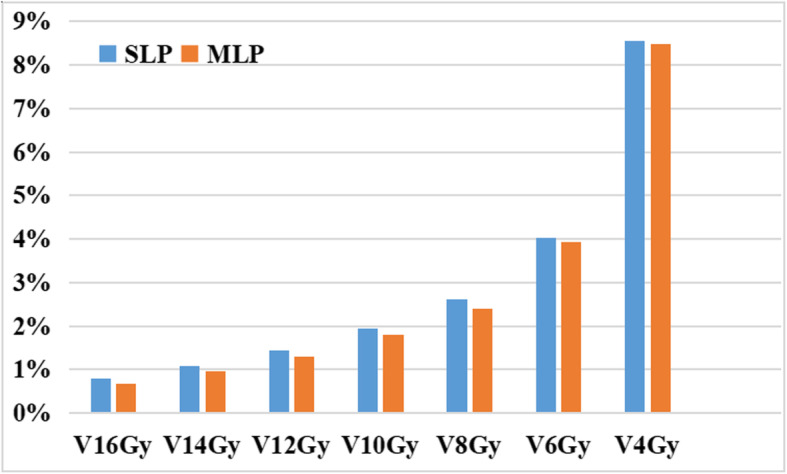
Results: Compared with those in the SLPs, the maximum dose (Dmax) and mean dose (Dmean) of brainstem in the MLP were reduced 0.22-3.13% (2.62%) and 2.71-12.56% (5.57%), respectively, all P < 0.05. Meanwhile, the volumes of the whole brain minus the tumors that received a single dose equivalent of 8-16 Gy (V8Gy-V16Gy) were effectively reduced in the MLP. The treatment time parameters, the total number of beams and monitor units, of the MLP were reduced by 3.31 and 1.47% (P < 0.05), respectively. Although there were a few differences in the conformity index (CI) and homogeneity index (HI) between the two treatment plans, the differences were not statistically significant (P = 2.94 and 1.08 > 0.05).
Conclusion: One multiple-lesions plan for brain metastases could achieve higher precision in the target and lower doses in healthy tissue while shortening the treatment time and improving the treatment efficiency over multiple single-lesion plans.
Keywords: Cyberknife; Multiple brain metastases; Multiple-lesions plan; Single-lesion plans.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Moore A, Cohen-Naftaly M, Tobar A, Kundel Y, Benjaminov O, Braun M, Issachar A, Mor E, Sarfaty M, Bragilovski D. Stereotactic body radiation therapy (SBRT) for definitive treatment and as a bridge to liver transplantation in early stage inoperable hepatocellular carcinoma. Radiat Oncol. 2017;12:163. doi: 10.1186/s13014-017-0899-4. - DOI - PMC - PubMed
-
- Tian J, Luo Y, Xiang J, Tang J. Combined treatment for non-small cell lung cancer and breast cancer patients with brain metastases with whole brain radiotherapy and temozolomide: a systematic review and meta-analysis. J Neuro-Oncol. 2017:1–11. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
