

A phase Ib/IIa, randomised, double-blind, multicentre trial to assess the safety and efficacy of expanded Cx611 allogeneic adipose-derived stem cells (eASCs) for the treatment of patients with community-acquired bacterial pneumonia admitted to the intensive care unit
- PMID: 33238991
- PMCID: PMC7686829
- DOI: 10.1186/s12890-020-01324-2
A phase Ib/IIa, randomised, double-blind, multicentre trial to assess the safety and efficacy of expanded Cx611 allogeneic adipose-derived stem cells (eASCs) for the treatment of patients with community-acquired bacterial pneumonia admitted to the intensive care unit
Abstract
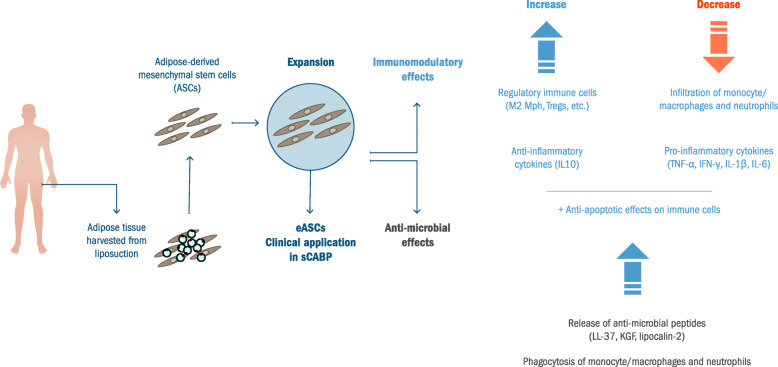
Background: Community-acquired bacterial pneumonia (CABP) can lead to sepsis and is associated with high mortality rates in patients presenting with shock and/or respiratory failure and who require mechanical ventilation and admission to intensive care units, thus reflecting the limited effectiveness of current therapy. Preclinical studies support the efficacy of expanded allogeneic adipose-derived mesenchymal stem cells (eASCs) in the treatment of sepsis. In this study, we aim to test the safety, tolerability and efficacy of eASCs as adjunctive therapy in patients with severe CABP (sCABP).
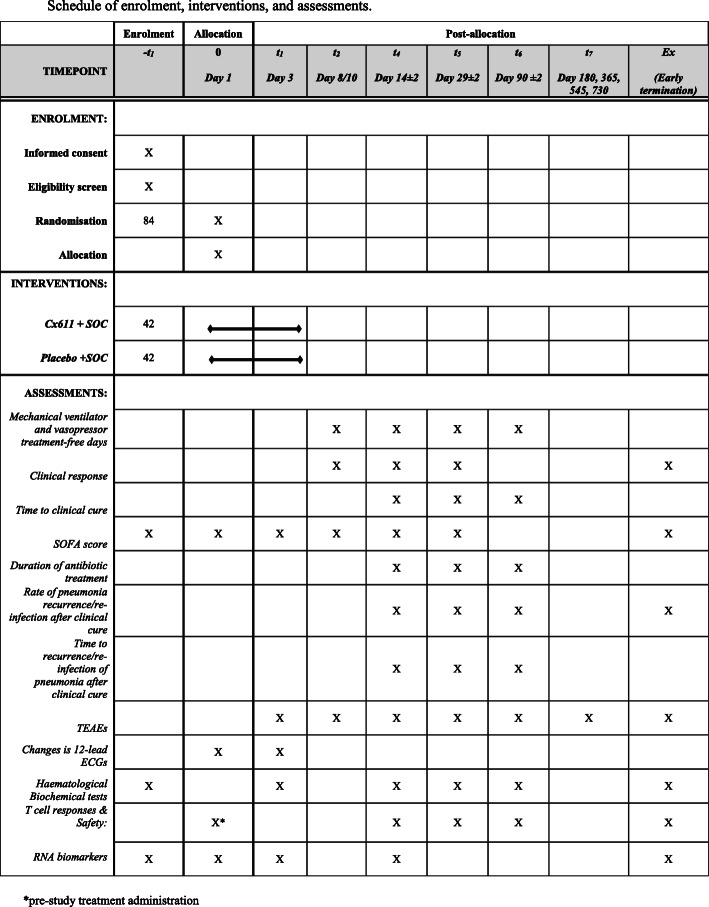
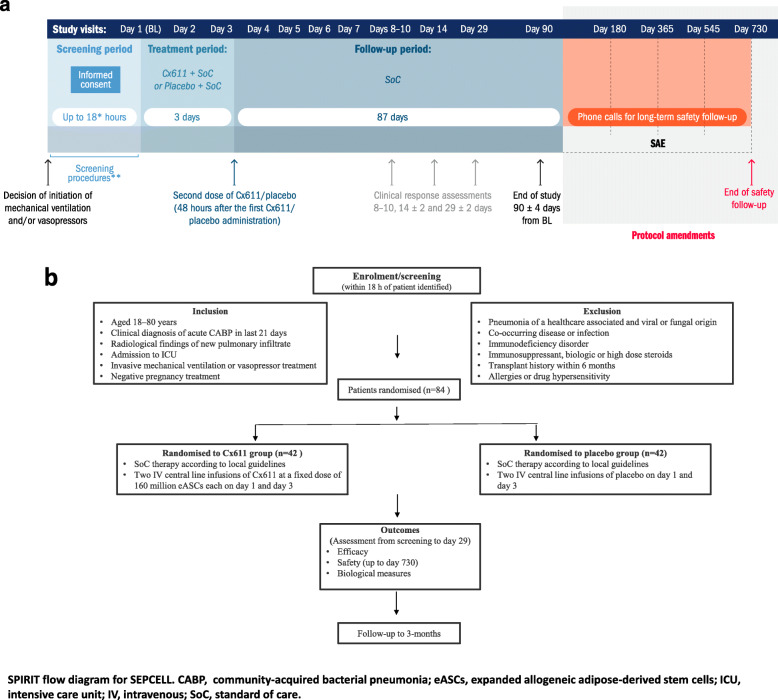
Methods: In addition to standard of care according to local guidelines, we will administer eASCs (Cx611) or placebo intravenously as adjunctive therapy to patients with sCABP. Enrolment is planned for approximately 180 patients who will be randomised to treatment groups in a 1:1 ratio according to a pre-defined randomization list. An equal number of patients is planned for allocation to each group. Cx611 will be administered on Day 1 and on Day 3 at a dose of 160 million cells (2 million cells / mL, total volume 80 mL) through a 20-30 min (240 mL/hr) intravenous (IV) central line infusion after dilution with Ringer Lactate solution. Placebo (Ringer Lactate) will also be administered through a 20-30 min (240 mL/hr) IV central line infusion at the same quantity (total volume of 80 mL) and following the same schedule as the active treatment. The study was initiated in January 2017 and approved by competent authorities and ethics committees in Belgium, Spain, Lithuania, Italy, Norway and France; monitoring will be performed at regular intervals. Funding is from the European Union's Horizon 2020 Research and Innovation Program.
Discussion: SEPCELL is the first trial to assess the effects of eASCs in sCABP. The data generated will advance understanding of the mode of action of Cx611 and will provide evidence on the safety, tolerability and efficacy of Cx611 in patients with sCABP. These data will be critical for the design of future confirmatory clinical investigations and will assist in defining endpoints, key biomarkers of interest and sample size determination.
Trial registration: NCT03158727 , retrospectively registered on 9 May 2017.
Keywords: Adjunctive therapy; Clinical trial; Community acquired bacterial pneumonia; Mesenchymal stem cells; Study protocol.
Conflict of interest statement
TvdP, PFL, MS and BF are members of the SEPCELL Consortium. OdlR, K-AC and EL are employees of Takeda. The institutions of PFL, MS and BF are study sites. In addition to funding from the European Union, Takeda Pharmaceuticals provided additional funding for the SEPCELL study.
Figures
References
-
- Liapikou A, Cilloniz C. Severe community-acquired pneumonia: severity and management. Community Acquir Infect. 2015;2:3. doi: 10.4103/2225-6482.153855. - DOI
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
