

Total cardiovascular or fatal events in people with type 2 diabetes and cardiovascular risk factors treated with dulaglutide in the REWIND trail: a post hoc analysis
- PMID: 33239067
- PMCID: PMC7690176
- DOI: 10.1186/s12933-020-01179-1
Total cardiovascular or fatal events in people with type 2 diabetes and cardiovascular risk factors treated with dulaglutide in the REWIND trail: a post hoc analysis
Abstract
Background: The Researching cardiovascular Events with a Weekly INcretin in Diabetes (REWIND) double blind randomized trial demonstrated that weekly subcutaneous dulaglutide 1.5 mg, a glucagon like peptide-1 receptor agonist, versus matched placebo reduced the first outcome of major adverse cardiovascular event (MACE), cardiovascular death, nonfatal myocardial infarction or nonfatal stroke (594 versus 663 events) in 9901 persons with type 2 diabetes and either chronic cardiovascular disease or risk factors, and followed during 5.4 years. These findings were based on a time-to-first-event analysis and preclude relevant information on the burden of total major events occurring during the trial. This analysis reports on the total cardiovascular or fatal events in the REWIND participants METHODS: We compared the total incidence of MACE or non-cardiovascular deaths, and the total incidence of expanded MACE (MACE, unstable angina, heart failure or revascularization) or non-cardiovascular deaths between participants randomized to dulaglutide and those randomized to placebo. Incidences were expressed as number per 1000 person-years. Hazard ratios (HR) were calculated using the conditional time gap and proportional means models.
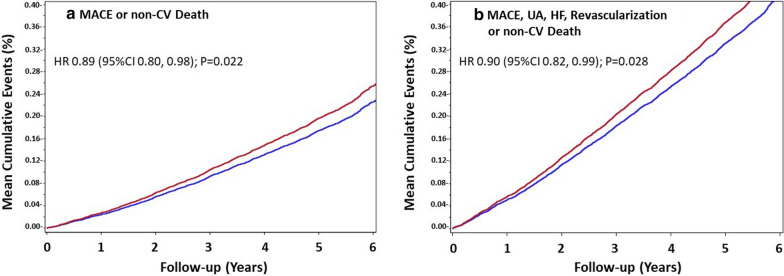
Results: Participants had a mean age of 66.2 years, 46.3% were women and 31% had previous cardiovascular disease. During the trial there were 1972 MACE or non-cardiovascular deaths and 3673 expanded MACE or non-cardiovascular deaths. The incidence of total MACE or non-cardiovascular deaths in the dulaglutide and placebo groups was 35.8 and 40.3 per 1000 person-years, respectively [absolute reduction = 4.5 per 1000 person-years; conditional time gap HR 0.90 (95% CI, 0.82-0.98) p = 0.020, and proportional means HR 0.89 (95% CI, 0.80-0.98) p = 0.022]. The incidence of total expanded MACE or non-cardiovascular deaths in the dulaglutide and placebo groups was 67.1 and 74.7 per 1000 person-years, respectively [absolute reduction = 7.6 per 1000 person-years; conditional time gap HR 0.93 (95% CI, 0.87-0.99) p = 0.023, and proportional means HR 0.90 (95% CI, 0.82-0.99) p = 0.028].
Conclusions: These findings suggest that weekly subcutaneous dulaglutide reduced total cardiovascular or fatal event burden in people with type 2 diabetes at moderate cardiovascular risk.
Clinical trial registration: https://www.clinicaltrials.gouv . Unique Identifier NCT01394952).
Keywords: Cardiovascular disease; Glucagon like peptide-1 receptor agonists; Type 2 diabetes.
Conflict of interest statement
GRD received honoraria from BAYER for lectures. LR received research grants from Swedish Heart–Lung Foundation, Stockholm County council, Family Erling Perssons Foundation and Boehringer-Ingelheim and speaker honoraria from Bayer AG, Boehringer-Ingelheim, Eli Lilly and Novo Nordisk. LAL received research grants from, provided CME on behalf of and/or acted as an adviser to AstraZeneca, Boehringer Ingelheim, Eli Lilly, GSK, Janssen, Lexicon, Merck, Novo Nordisk, Sanofi, and Servier. ML is employed by Eli Lilly. LD has no competing interests. JLP has no competing interests. CMA is employed by Eli Lilly. JES has received honoraria from AstraZeneca, Merck Sharp & Dohme Corp., Mylan, Sanofi. Eli Lilly, Novo Nordisk and Boehringer Ingelheim. IC has received honoraria for lectures and consulting fees from Abbot, Medtronic, Bayer, GlaxoSmithKline, Eli Lilly, Novo Nordisk, Sanofi-Aventis, Novartis and MSD. WCCPLJ has received honoraria for speaking from Merck, Menarini, Sanofi, Abbott, WCC has received institutional grant support from Eli Lilly. FL has no competing interests. EGCM acted as an adviser for Servier and received honoraria from Menarini, Sanofi, MSD, Silanes, Novo, Stendhal, Boryun for lectures. VP has no competing interests. NP has no competing interests. JB received research grants from Eli Lilly, ReCor, and Ablative Solutions. He is a consultant for both Medtronic and Up-to-Date. WHHS provided CME and/or acted as an adviser to MSD, AstraZeneca, Boehringer Ingelheim, Tanabe, Takeda, Eli Lilly, Bayer’s, Novo Nordisk, and Sanofi. TTK has no competing interests. PJR has no competing interests. MK has no competing interests. SH has no competing interests. PP has no competing interest. HMC has received grants from Eli Lilly, AstraZeneca, Regeneron, Pfizer, Novo Nordisk, honoraria for speaker bureau from Eli Lilly and advisory panel from Sanofi Aventis and Novartis, and is shareholder Roche Pharma. MCR reports grant support through Oregon Health & Science University from Astra Zeneca, Eli Lilly, and Novo Nordisk, and honoraria for consulting from Adocia, AstraZeneca, Eli Lilly, GlaxoSmithKline, Intercept, Novo Nordisk, Sanofi, and Theracos. HCG holds the McMaster-Sanofi Population Health Institute Chair in Diabetes Research and Care. He reports research grants from Eli Lilly, AstraZeneca, Merck, Novo Nordisk and Sanofi; honoraria for speaking from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk, and Sanofi; and consulting fees from Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck, Novo Nordisk, Janssen, Sanofi, and Kowa.
Figures
References
-
- Hernandez AF, Green JB, Janmohamed S, D’Agostino RB, Granger CB, Jones NP, et al. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomized placebo-controlled trial. Lancet. 2018;392(10157):1519–1529. doi: 10.1016/S0140-6736(18)32261-X. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
