

Discordance between patient and physician global assessment of disease activity in Behçet's syndrome: a multicenter study cohort
- PMID: 33239083
- PMCID: PMC7687797
- DOI: 10.1186/s13075-020-02362-1
Discordance between patient and physician global assessment of disease activity in Behçet's syndrome: a multicenter study cohort
Abstract
Background: To compare the patients' and physician's global assessment of disease activity in Behçet's syndrome (BS) and investigate the frequency, magnitude, and determinants of potential discordance.
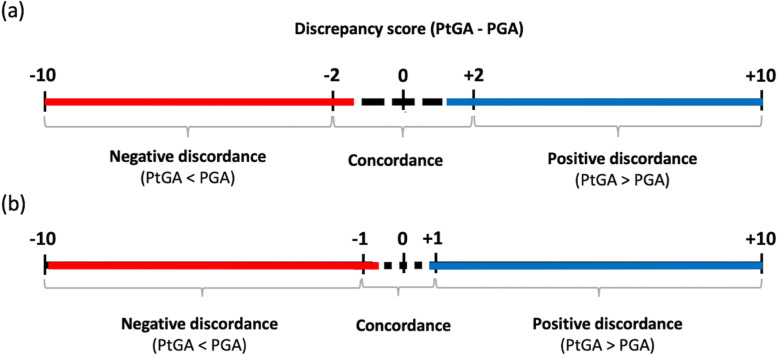
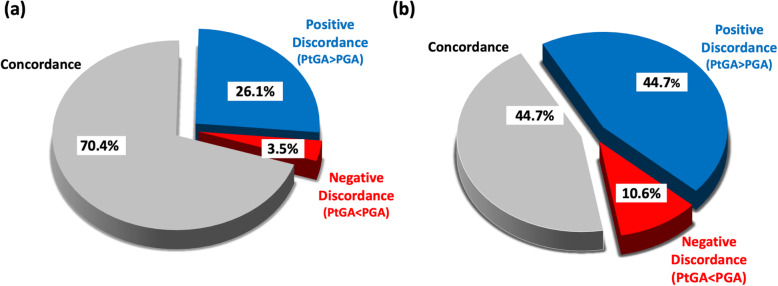
Methods: A total of 226 adult BS patients with a median (IQR) age of 46.9 (35.6-55.2) years were enrolled across Italy, Greece, Portugal, and Spain. Demographic, clinical, and therapeutic variables, as well as the patient reported outcomes, were collected at the recruitment visit. The physical (PCS) and mental (MCS) component summary scores of the Short Form Questionnaire 36 (SF-36) and the Behçet's syndrome Overall Damage Index (BODI) were calculated. Disease activity was assessed by the patients' (PtGA) and physician's global assessment (PGA) in a 10-cm visual analog scale, as well as the Behçet Disease Current Activity Form (BDCAF). Discordance (∆) was calculated by subtracting the PGA from the PtGA and defined as positive (PtGA>PGA) and negative (PtGA<PGA) discordance using both a more stringent (∆ = ±2) and a less stringent (∆ = ±1) cutoff. Univariate and multivariate logistic regressions were performed.
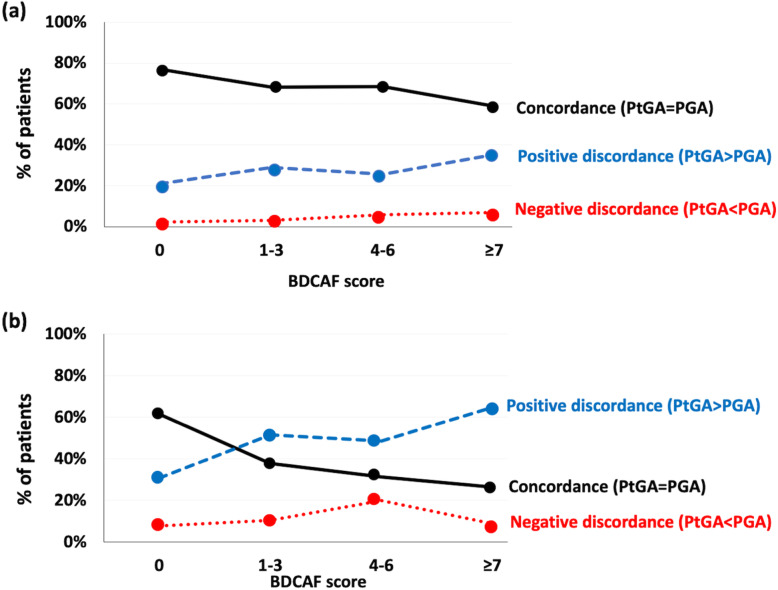
Results: Median PtGA and PGA scores were 2.0 (0.3-5.0) and 1.0 (0.0-3.0) cm, respectively. The discordance prevalence varied (from 29.6 to 55.3%) according to the cutoff applied, and the majority (> 80%) of disagreements were due to patients rating higher their disease activity. Higher values of BDCAF were associated to increased rate of positive discordance. When BDCAF = 0, the median (IQR) values of PtGA and PGA were 0.2 (0-2) and 0 (0-1), respectively. PCS (adjusted odds ratio (adjOR) 0.96 per unit, 95% CI 0.93-0.98, p = 0.006) and MCS (adjOR 0.96 per unit, 95% CI 0.93-0.99, p = 0.003) were independently associated with positive discordance using both cutoffs. Active ocular involvement emerged as a potential determinant of negative discordance (adjOR 5.88, 95% CI 1.48-23.30, p = 0.012).
Conclusions: PtGA and PGA should be considered as complementary measures in BS, as patients and physicians may be influenced by different factors when assessing active disease manifestations. Particularly, PtGA may be a useful tool in the assessment of BS disease activity, as it carries a low risk to misclassify an inactive disease, and may allow to capture aspects of the patient's health that negatively affect his well-being and the treatment.
Keywords: Behçet’s syndrome; Disease activity; Outcome measure; Patients reported outcomes.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Piga M, Mathieu A. The origin of Behçet’s disease geoepidemiology: possible role of a dual microbial-driven genetic selection. Clin Exp Rheumatol. 2014;32:S123–S129. - PubMed
