

Antibiotic therapeutic drug monitoring in intensive care patients treated with different modalities of extracorporeal membrane oxygenation (ECMO) and renal replacement therapy: a prospective, observational single-center study
- PMID: 33239110
- PMCID: PMC7689974
- DOI: 10.1186/s13054-020-03397-1
Antibiotic therapeutic drug monitoring in intensive care patients treated with different modalities of extracorporeal membrane oxygenation (ECMO) and renal replacement therapy: a prospective, observational single-center study
Abstract
Background: Effective antimicrobial treatment is key to reduce mortality associated with bacterial sepsis in patients on intensive care units (ICUs). Dose adjustments are often necessary to account for pathophysiological changes or renal replacement therapy. Extracorporeal membrane oxygenation (ECMO) is increasingly being used for the treatment of respiratory and/or cardiac failure. However, it remains unclear whether dose adjustments are necessary to avoid subtherapeutic drug levels in septic patients on ECMO support. Here, we aimed to evaluate and comparatively assess serum concentrations of continuously applied antibiotics in intensive care patients being treated with and without ECMO.
Methods: Between October 2018 and December 2019, we prospectively enrolled patients on a pneumological ICU in southwest Germany who received antibiotic treatment with piperacillin/tazobactam, ceftazidime, meropenem, or linezolid. All antibiotics were applied using continuous infusion, and therapeutic drug monitoring of serum concentrations (expressed as mg/L) was carried out using high-performance liquid chromatography. Target concentrations were defined as fourfold above the minimal inhibitory concentration (MIC) of susceptible bacterial isolates, according to EUCAST breakpoints.
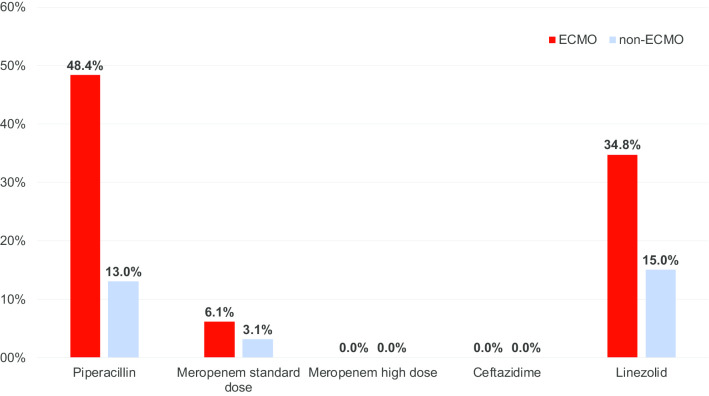
Results: The final cohort comprised 105 ICU patients, of whom 30 were treated with ECMO. ECMO patients were significantly younger (mean age: 47.7 vs. 61.2 years; p < 0.001), required renal replacement therapy more frequently (53.3% vs. 32.0%; p = 0.048) and had an elevated ICU mortality (60.0% vs. 22.7%; p < 0.001). Data on antibiotic serum concentrations derived from 112 measurements among ECMO and 186 measurements from non-ECMO patients showed significantly lower median serum concentrations for piperacillin (32.3 vs. 52.9; p = 0.029) and standard-dose meropenem (15.0 vs. 17.8; p = 0.020) in the ECMO group. We found high rates of insufficient antibiotic serum concentrations below the pre-specified MIC target among ECMO patients (piperacillin: 48% vs. 13% in non-ECMO; linezolid: 35% vs. 15% in non-ECMO), whereas no such difference was observed for ceftazidime and meropenem.
Conclusions: ECMO treatment was associated with significantly reduced serum concentrations of specific antibiotics. Future studies are needed to assess the pharmacokinetic characteristics of antibiotics in ICU patients on ECMO support.
Keywords: Antibiotics; Bacteremia; Diagnosis; Infection; Multiresistant bacteria; Sepsis; Therapeutic drug monitoring.
Conflict of interest statement
S. L. Becker has received travel grants and speaker fees from Astellas Pharmaceuticals, Becton Dickinson, Novartis and Pfizer, and participated at Advisory Boards by Pfizer and Shionogi. All other authors have nothing to disclose.
Figures
References
-
- Ferrer R, Martin-Loeches I, Phillips G, Osborn TM, Townsend S, Dellinger RP, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42:1749–1755. doi: 10.1097/CCM.0000000000000330. - DOI - PubMed
-
- Vazquez-Guillamet C, Scolari M, Zilberberg MD, Shorr AF, Micek ST, Kollef M. Using the number needed to treat to assess appropriate antimicrobial therapy as a determinant of outcome in severe sepsis and septic shock. Crit Care Med. 2014;42:2342–2349. doi: 10.1097/CCM.0000000000000516. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
