

NHS Health Checks for people with mental ill-health 2013-2017: an observational study
- PMID: 33239117
- PMCID: PMC7737190
- DOI: 10.1017/S2045796020001006
NHS Health Checks for people with mental ill-health 2013-2017: an observational study
Abstract
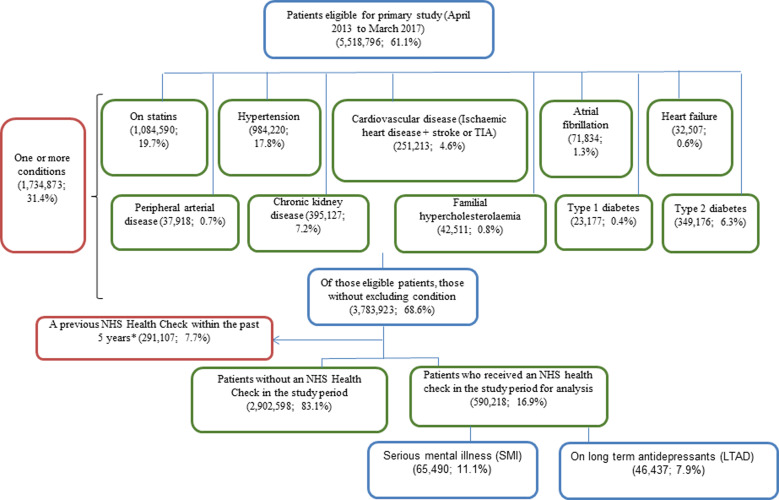
Aims: People living with serious mental ill-health experience adverse cardiovascular outcomes causing some of the greatest health inequality gaps in England, UK. We describe uptake of the NHS Health Check programme in people with mental ill-health, and rates of new diagnoses and management of cardiovascular risk factors in those who attend NHS Health Checks in comparison to those people without mental ill-health.
Methods: We used a large nationally representative database of people registered with general practitioners in England (QResearch). Between 2013 and 2017, we analysed attendance at NHS Health Checks and outcomes in the succeeding 12 months, in people with serious mental illness (SMI) including psychoses and in people prescribed long-term antidepressant medications (LTAD), with comparison to attendees who did not have these conditions. Hazard ratios (HR) were used to describe the association between outcomes and SMI and LTAD adjusting for sociodemographic variables.
Results: In those eligible for the NHS Health Check programme, we found a higher percentage of people with SMI attended an NHS Health Check (65 490, 19.8%) than those without SMI (524 728, 16.6%); adjusted HR 1.05 [95% confidence interval 1.02-1.08]. We also observed a higher percentage of attendance in people on LTAD (46 437, 20.1%) compared to people who were not prescribed LTAD (543 781, 16.7%); adjusted HR 1.10 (1.08-1.13). People with SMI were more likely to be identified with chronic kidney disease (CKD, HR 1.23, 1.12-1.34) and type 2 diabetes (HR 1.14, 1.03-1.25) within the 12 months following their NHS Health Check compared with those without SMI. People on LTAD were more likely to be identified with CKD (HR 1.55, 1.42-1.70) and type 2 diabetes (HR 1.45, 1.31-1.60) and also hypertension, cardiovascular disease, non-diabetic hyperglycaemia, familial hypercholesterolemia and dementia within the 12 months following their NHS Health Check. Statins were more likely to be prescribed to NHS Health Check attendees with SMI and those on LTAD than those without these conditions; HR 1.31 (1.25-1.38) and 1.91 (1.82-2.01), respectively. Antihypertensives were more likely to be prescribed to those on LTAD; HR 1.21 (1.14-1.29).
Conclusions: We found evidence that people with SMI or on LTAD treatment were 5-10% more likely to access NHS Health Checks than people without these conditions. People with SMI or on LTAD treatment who attended NHS Health Checks had higher rates of diagnosis of CKD, type 2 diabetes and some other relevant co-morbidities and increased treatment with statins and also anti-hypertensive medication in people on LTAD. This is likely to contribute to equitable reduction in adverse cardiovascular events for people with mental ill-health.
Keywords: Antidepressants; epidemiology; health service research; mental health; primary care.
Conflict of interest statement
All authors have completed the Unified Competing Interests form at
Figures
References
-
- Blackburn R, Osborn D, Walters K, Nazareth I and Petersen I (2018) Statin prescribing for prevention of cardiovascular disease amongst people with severe mental illness: cohort study in UK primary care. Schizophrenia Research 192, 219–225. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
