

Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral Toxoplasmosis
- PMID: 33239310
- PMCID: PMC7690944
- DOI: 10.1128/CMR.00115-19
Epidemiology, Pathophysiology, Diagnosis, and Management of Cerebral Toxoplasmosis
Abstract
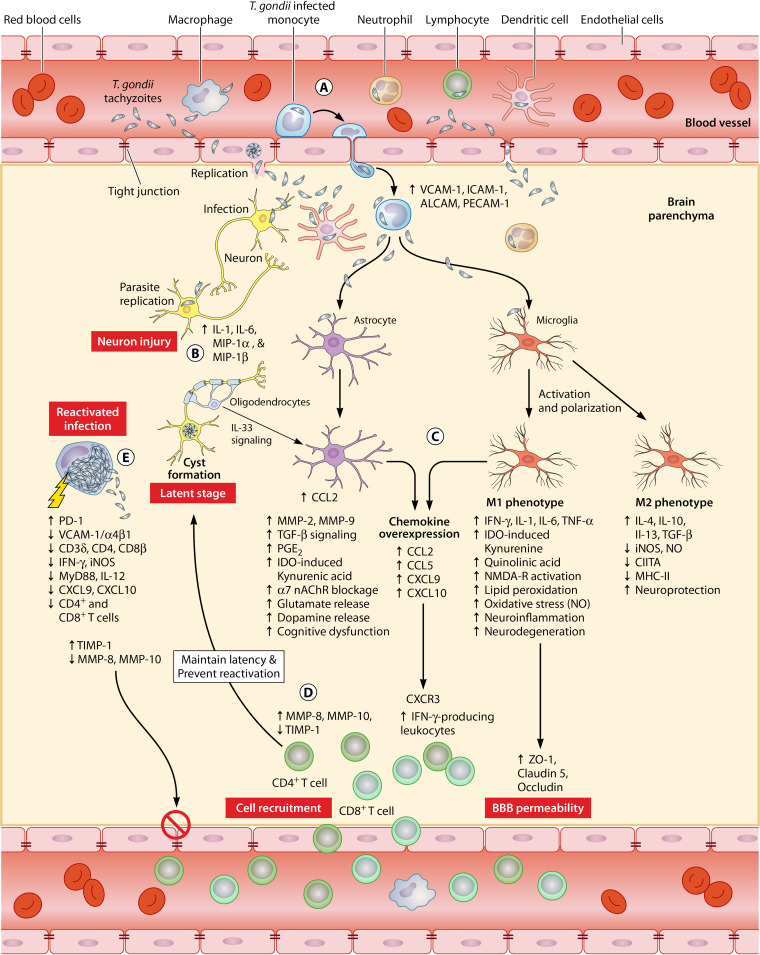
Toxoplasma gondii is known to infect a considerable number of mammalian and avian species and a substantial proportion of the world's human population. The parasite has an impressive ability to disseminate within the host's body and employs various tactics to overcome the highly regulatory blood-brain barrier and reside in the brain. In healthy individuals, T. gondii infection is largely tolerated without any obvious ill effects. However, primary infection in immunosuppressed patients can result in acute cerebral or systemic disease, and reactivation of latent tissue cysts can lead to a deadly outcome. It is imperative that treatment of life-threatening toxoplasmic encephalitis is timely and effective. Several therapeutic and prophylactic regimens have been used in clinical practice. Current approaches can control infection caused by the invasive and highly proliferative tachyzoites but cannot eliminate the dormant tissue cysts. Adverse events and other limitations are associated with the standard pyrimethamine-based therapy, and effective vaccines are unavailable. In this review, the epidemiology, economic impact, pathophysiology, diagnosis, and management of cerebral toxoplasmosis are discussed, and critical areas for future research are highlighted.
Keywords: Toxoplasma gondii; cerebral toxoplasmosis; diagnosis; immunocompromised patients; pathophysiology; toxoplasmic encephalitis; treatment.
Copyright © 2020 American Society for Microbiology.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
