

Sampling interstitial fluid from human skin using a microneedle patch
- PMID: 33239384
- PMCID: PMC7871333
- DOI: 10.1126/scitranslmed.aaw0285
Sampling interstitial fluid from human skin using a microneedle patch
Abstract
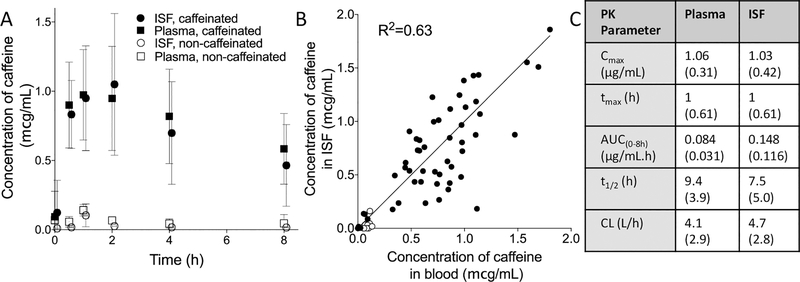
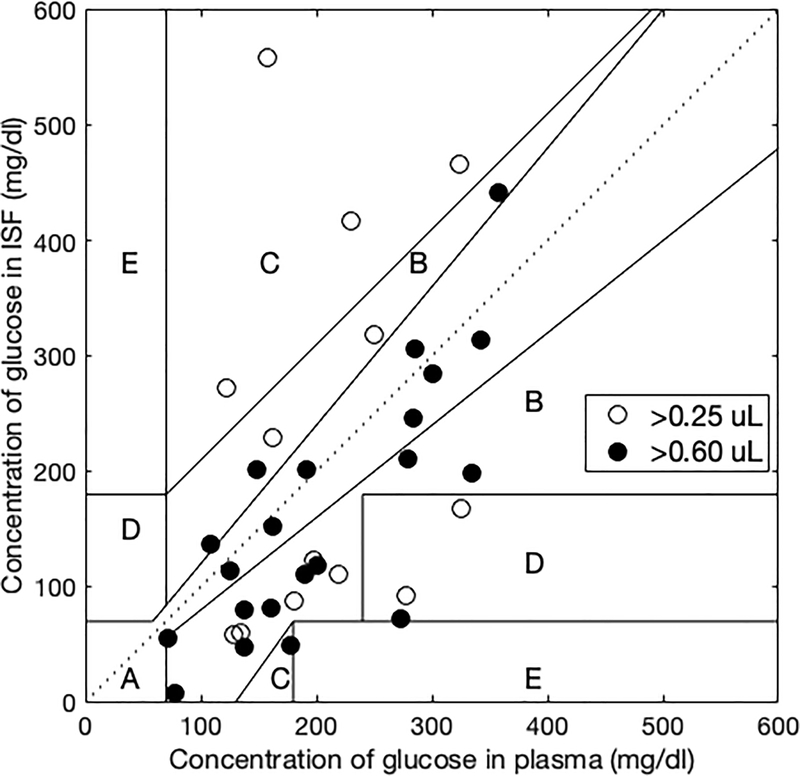
Tissue interstitial fluid (ISF) surrounds cells and is an underutilized source of biomarkers that complements conventional sources such as blood and urine. However, ISF has received limited attention due largely to lack of simple collection methods. Here, we developed a minimally invasive, microneedle-based method to sample ISF from human skin that was well tolerated by participants. Using a microneedle patch to create an array of micropores in skin coupled with mild suction, we sampled ISF from 21 human participants and identified clinically relevant and sometimes distinct biomarkers in ISF when compared to companion plasma samples based on mass spectrometry analysis. Many biomarkers used in research and current clinical practice were common to ISF and plasma. Because ISF does not clot, these biomarkers could be continuously monitored in ISF similar to current continuous glucose monitors but without requiring an indwelling subcutaneous sensor. Biomarkers distinct to ISF included molecules associated with systemic and dermatological physiology, as well as exogenous compounds from environmental exposures. We also determined that pharmacokinetics of caffeine in healthy adults and pharmacodynamics of glucose in children and young adults with diabetes were similar in ISF and plasma. Overall, these studies provide a minimally invasive method to sample dermal ISF using microneedles and demonstrate human ISF as a source of biomarkers that may enable research and translation for future clinical applications.
Copyright © 2020 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Figures

References
-
- Downing GJ, in Pharmaceutical Sciences Encyclopedia. (John Wiley & Sons, Inc, 2010).
-
- Fischbach FT, Dinning MB, A manual of laboratory and diagnostic tests. (Wolters Kluwer Health, ed. 8th edition, 2009), pp. 1283.
-
- Fogh-Andersen N, Altura BM, Altura BT, Siggaard-Andersen O, Composition of interstitial fluid. Clinical chemistry 41, 1522–1525 (1995); published online EpubOct ( - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
