

Plaque morphology in acute symptomatic intracranial atherosclerotic disease
- PMID: 33239439
- PMCID: PMC7958085
- DOI: 10.1136/jnnp-2020-325027
Plaque morphology in acute symptomatic intracranial atherosclerotic disease
Abstract
Background: Intracranial atherosclerotic disease (ICAD) is globally a major ischaemic stroke subtype with high recurrence. Understanding the morphology of symptomatic ICAD plaques, largely unknown by far, may help identify vulnerable lesions prone to relapse.
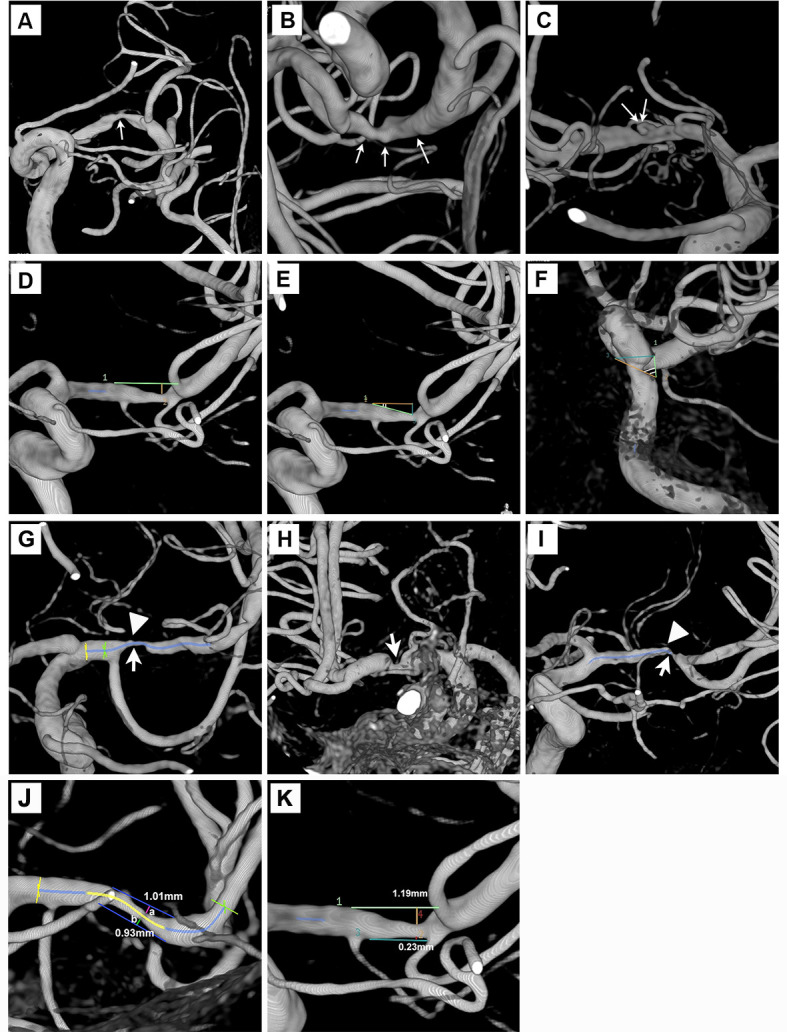
Methods: We prospectively recruited patients with acute ischaemic stroke or transient ischaemic attack attributed to high-grade ICAD (60%-99% stenosis). Plaque morphological parameters were assessed in three-dimensional rotational angiography, including surface contour, luminal stenosis, plaque length/thickness, upstream shoulder angulation, axial/longitudinal plaque distribution and presence of adjoining branch atheromatous disease (BAD). We compared morphological features of smooth, irregular and ulcerative plaques and correlated them with cerebral ischaemic lesion load downstream in MRI.
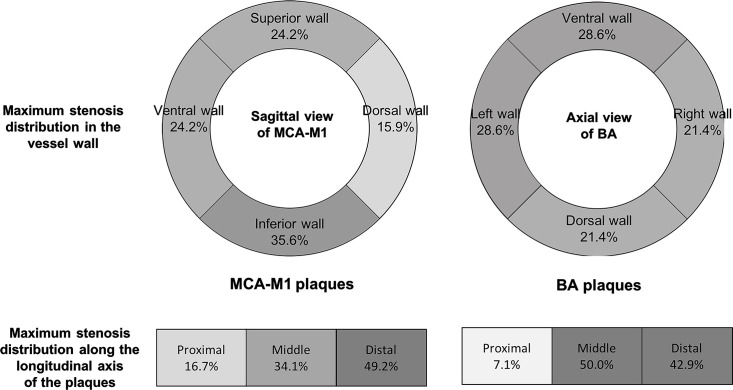
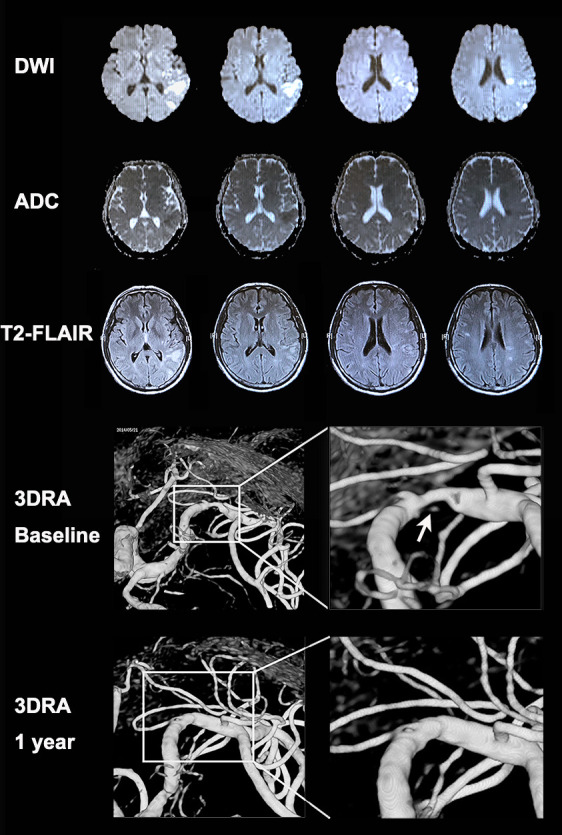
Results: Among 180 recruited patients (median age=60 years; 63.3% male; median stenosis=75%), plaque contour was smooth (51 (28.3%)), irregular (101 (56.1%)) or ulcerative (28 (15.6%)). Surface ulcers were mostly at proximal (46.4%) and middle one-third (35.7%) of the lesions. Most (84.4%) plaques were eccentric, and half had their maximum thickness over the distal end. Ulcerative lesions were thicker (medians 1.6 vs 1.3 mm; p=0.003), had steeper upstream shoulder angulation (56.2° vs 31.0°; p<0.001) and more adjoining BAD (83.3% vs 57.0%; p=0.033) than non-ulcerative plaques. Ulcerative plaques were significantly associated with coexisting acute and chronic infarcts downstream (35.7% vs 12.5%; adjusted OR 4.29, 95% CI 1.65 to 11.14, p=0.003). Sensitivity analyses in patients with anterior-circulation ICAD lesions showed similar results in the associations between the plaque types and infarct load.
Conclusions: Ulcerative intracranial atherosclerotic plaques were associated with vulnerable morphological features and had a higher cumulative infarct load downstream.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Rothwell PM, Gibson R, Warlow CP, et al. . Interrelation between plaque surface morphology and degree of stenosis on carotid angiograms and the risk of ischemic stroke in patients with symptomatic carotid stenosis. on behalf of the European carotid surgery Trialists' Collaborative group. Stroke 2000;31:615–21. 10.1161/01.str.31.3.615 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Medical
Research Materials