

Cutaneous and systemic granulomatosis in ataxia-telangiectasia: a clinico-pathological study
- PMID: 33240017
- PMCID: PMC7675092
- DOI: 10.5114/ada.2020.100485
Cutaneous and systemic granulomatosis in ataxia-telangiectasia: a clinico-pathological study
Abstract
Introduction: The development of granulomas is a well-recognized manifestation of immunodeficiency in ataxia-telangiectasia (A-T), resulting from lymphocyte developmental abnormalities, impaired immunosurveillance, and inappropriate innate immune response-driven inflammation.
Aim: To better understand pathological and immunological phenomena involved in development of cutaneous and visceral granulomatosis observable in patients with ataxia-telangiectasia.
Material and methods: We retrospectively reviewed medical records of eight A-T children, aged from 2 to 13 years, with regard to clinical, immunological and histopathological features of cutaneous and visceral granulomatosis.
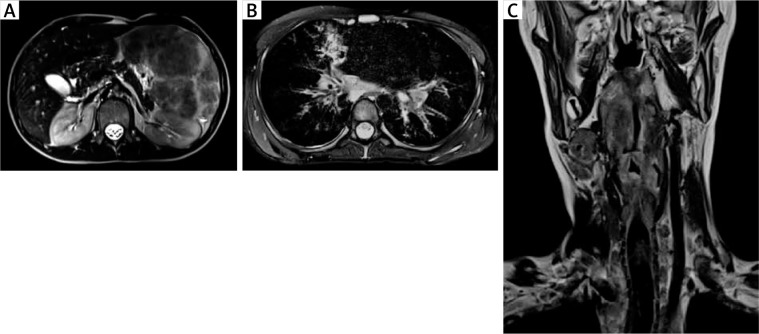
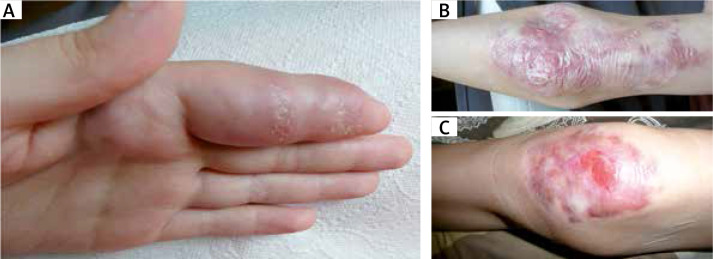
Results: In four out of eight A-T patients studied, cutaneous granulomas clinically presented as skin nodules and ulcerated erythematous plaques disseminated on the face, and on trauma-prone areas of upper and lower extremities. Visceral granulomatosis had a severe clinical course and involved the lungs, the spleen, the liver and the larynx. Histologically, cutaneous and laryngeal granulomas showed extensive cellular infiltrations containing T lymphocytes with predominating CD8+ phenotype and with CD68+ histiocytes. The immunological profile with the hyper-IgM phenotype, markedly reduced numbers of B and naive CD4+ and CD8+ T cells with predominating IgM-only memory B cells and skewed repertoire of a T cell receptor was observable in patients with skin and visceral granulomatosis.
Conclusions: In the setting of combined immunodeficiency in A-T, cutaneous and systemic granulomatosis reflects a granulomatous reaction pattern, as a result of inappropriate immune regulation.
Keywords: ataxia-telangiectasia; children; granuloma; immunodeficiency; lymphopenia.
Copyright © 2020 Termedia.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Driessen GJ, Ijspeert H, Weemaes CM, et al. . Antibody deficiency in patients with ataxia telangiectasia is caused by disturbed B-and T-cell homeostasis and reduced repertoire diversity. J Allergy Clin Immmunol 2013; 131: 1367-75. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials