

Added Prognostic Value of Hemorrhagic Transformation Quantification in Patients With Acute Ischemic Stroke
- PMID: 33240206
- PMCID: PMC7683432
- DOI: 10.3389/fneur.2020.582767
Added Prognostic Value of Hemorrhagic Transformation Quantification in Patients With Acute Ischemic Stroke
Abstract
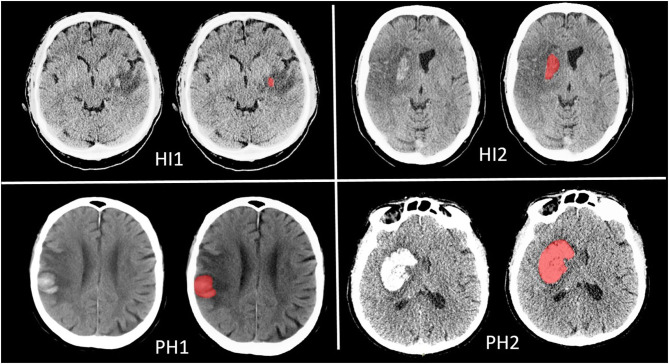
Introduction and Aim: Hemorrhagic transformation (HT) frequently occurs after acute ischemic stroke and negatively influences the functional outcome. Usually, HT is classified by its radiological appearance. Discriminating between the subtypes can be complicated, and interobserver variation is considerable. Therefore, we aim to quantify rather than classify hemorrhage volumes and determine the association of hemorrhage volume with functional outcome in comparison with the European Cooperative Acute Stroke Study II classification. Patients and Methods: We included patients from the MR CLEAN trial with follow-up imaging. Hemorrhage volume was estimated by manual delineation of the lesion, and HT was classified according to the European Cooperative Acute Stroke Study II classification [petechial hemorrhagic infarction types 1 (HI1) and 2 (HI2) and parenchymal hematoma types 1 (PH1) and 2 (PH2)] on follow-up CT 24 h to 2 weeks after treatment. We assessed functional outcome using the modified Rankin Scale 90 days after stroke onset. Ordinal logistic regression with and without adjustment for potential confounders was used to describe the association of hemorrhage volume with functional outcome. We created regression models including and excluding total lesion volume as a confounder. Results: We included 478 patients. Of these patients, 222 had HT. Median hemorrhage volume was 3.37 ml (0.80-12.6) and per HT subgroup; HI1: 0.2 (0.0-1.7), HI2: 3.2 (1.7-6.1), PH1: 6.3 (4.2-13), and PH2: 47 (19-101). Hemorrhage volume was associated with functional outcome [adjusted common odds ratio (acOR): 0.83, 95% CI: 0.73-0.95] but not anymore after adjustment for total lesion volume (acOR: 0.99, 95% CI: 0.86-1.15, per 10 ml). Hemorrhage volume in patients with PH2 was significantly associated with functional outcome after adjusting total lesion volume (acOR: 0.70, 95% CI: 0.50-0.98). Conclusion: HT volume is associated with functional outcomes in patients with acute ischemic stroke but not independent of total lesion volume. The extent of a PH2 was associated with outcome, suggesting that measuring hemorrhage volume only provides an additional benefit in the prediction of the outcome when a PH2 is present.
Keywords: endovascular therapy (EVT); hemorrhage volume; hemorrhagic transformation (HT); intracranial hemorrhage (ICH); ischemic stroke (IS); thrombolysis.
Copyright © 2020 van Kranendonk, Treurniet, Boers, Berkhemer, Coutinho, Lingsma, van Zwam, van der Lugt, van Oostenbrugge, Dippel, Roos, Marquering, Majoie and the MR CLEAN investigators.
Figures



References
-
- van Kranendonk KR, Treurniet KM, Boers AMM, Berkhemer OA, van den Berg LA, Chales V, et al. . Hemorrhagic transformation is associated with poor functional outcome in patients with acute ischemic stroke due to a large vessel occlusion. J Neurointerv Surg. (2019) 11:464–8. 10.1136/neurintsurg-2018-014141 - DOI - PubMed
LinkOut - more resources
Full Text Sources