

Interventions to reduce medication errors in adult medical and surgical settings: a systematic review
- PMID: 33240478
- PMCID: PMC7672746
- DOI: 10.1177/2042098620968309
Interventions to reduce medication errors in adult medical and surgical settings: a systematic review
Abstract
Background and aims: Medication errors occur at any point of the medication management process, and are a major cause of death and harm globally. The objective of this review was to compare the effectiveness of different interventions in reducing prescribing, dispensing and administration medication errors in acute medical and surgical settings.
Methods: The protocol for this systematic review was registered in PROSPERO (CRD42019124587). The library databases, MEDLINE, CINAHL, EMBASE, PsycINFO, Cochrane Database of Systematic Reviews and the Cochrane Central Register of Controlled Trials were searched from inception to February 2019. Studies were included if they involved testing of an intervention aimed at reducing medication errors in adult, acute medical or surgical settings. Meta-analyses were performed to examine the effectiveness of intervention types.
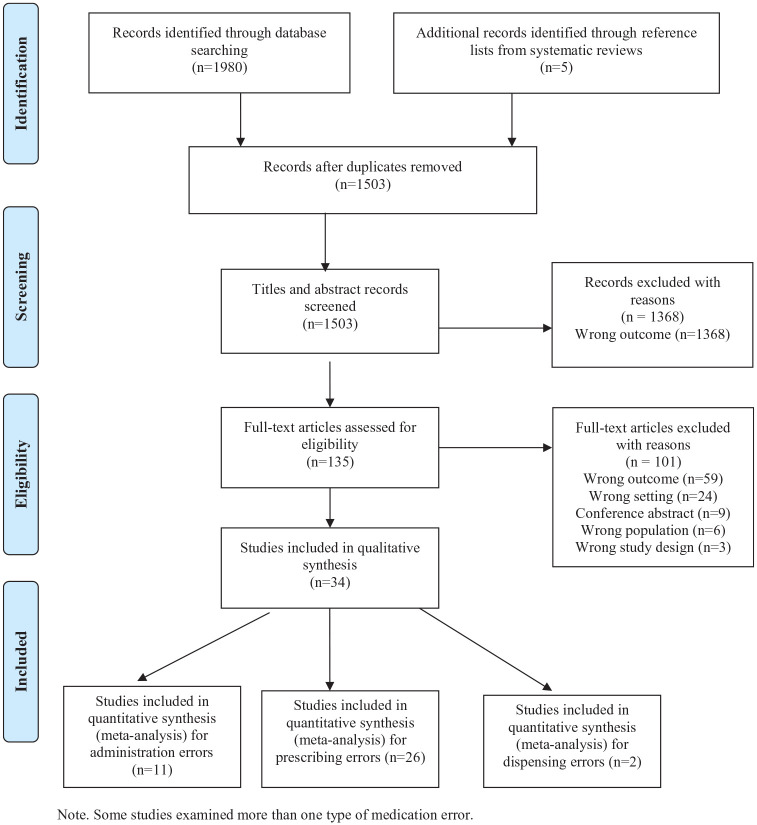
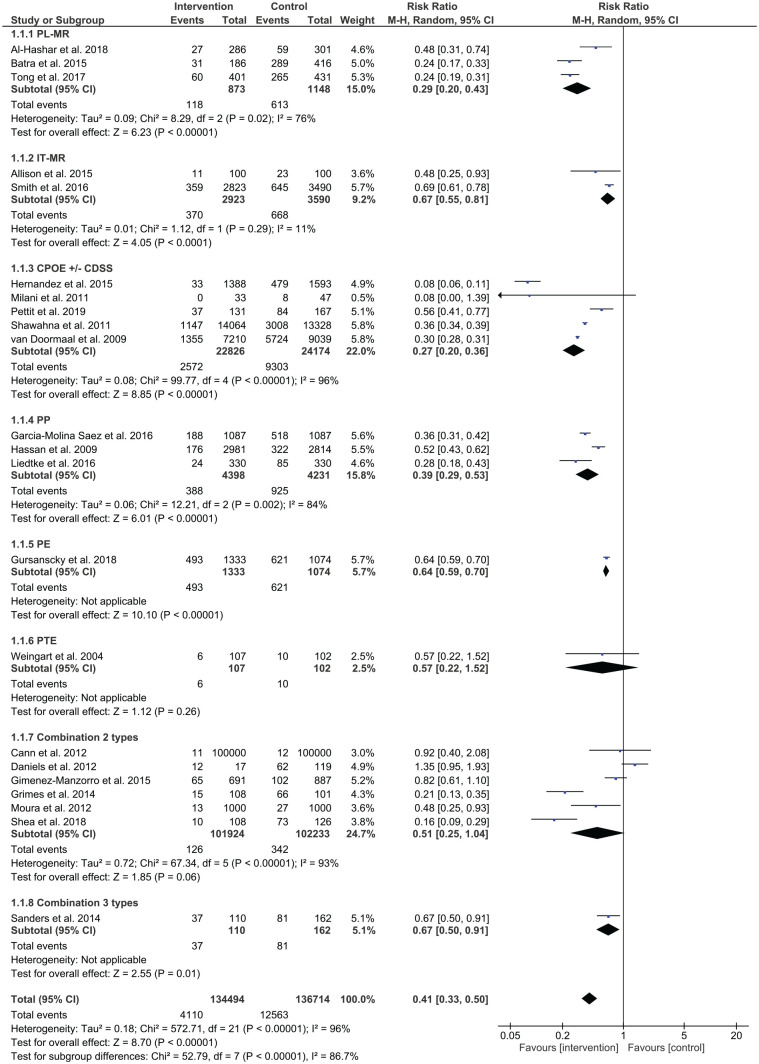
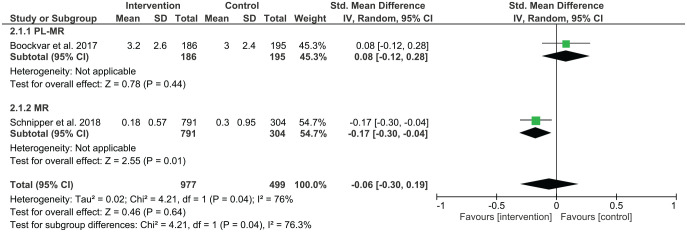
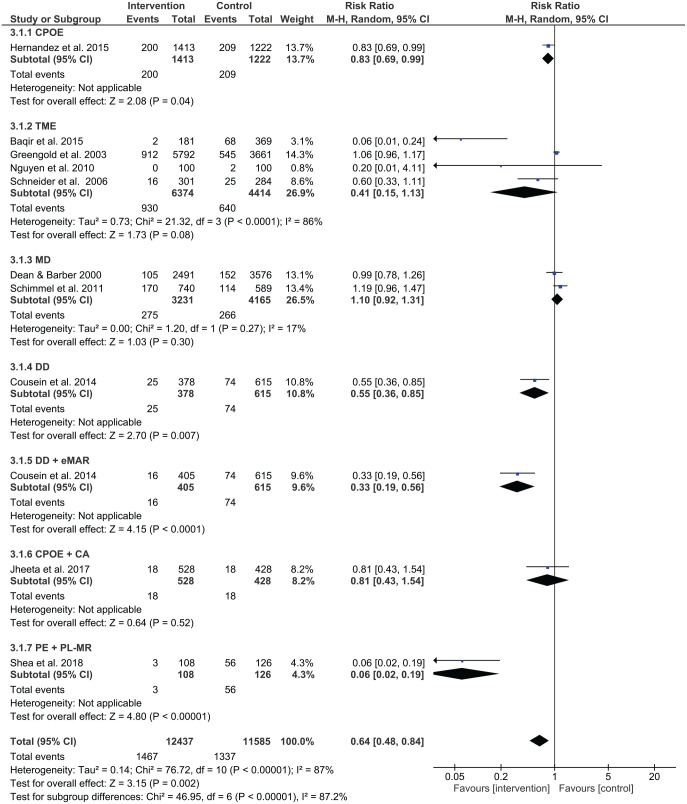
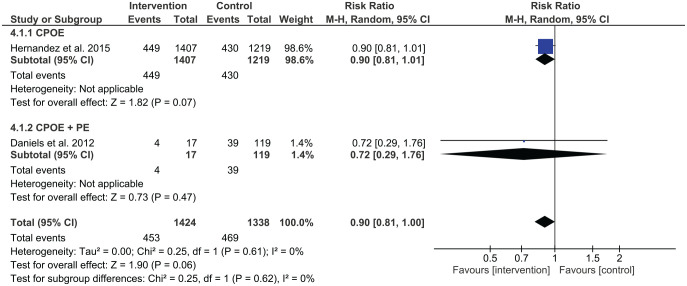
Results: A total of 34 articles were included with 12 intervention types identified. Meta-analysis showed that prescribing errors were reduced by pharmacist-led medication reconciliation, computerised medication reconciliation, pharmacist partnership, prescriber education, medication reconciliation by trained mentors and computerised physician order entry (CPOE) as single interventions. Medication administration errors were reduced by CPOE and the use of an automated drug distribution system as single interventions. Combined interventions were also found to be effective in reducing prescribing or administration medication errors. No interventions were found to reduce dispensing error rates. Most studies were conducted at single-site hospitals, with chart review being the most common method for collecting medication error data. Clinical significance of interventions was examined in 21 studies. Since many studies were conducted in a pre-post format, future studies should include a concurrent control group.
Conclusion: The systematic review identified a number of single and combined intervention types that were effective in reducing medication errors, which clinicians and policymakers could consider for implementation in medical and surgical settings. New directions for future research should examine interdisciplinary collaborative approaches comprising physicians, pharmacists and nurses.
Lay summary: Activities to reduce medication errors in adult medical and surgical hospital areas.
Introduction: Medication errors or mistakes may happen at any time in hospital, and they are a major reason for death and harm around the world.
Objective: To compare the effectiveness of different activities in reducing medication errors occurring with prescribing, giving and supplying medications in adult medical and surgical settings in hospital.
Methods: Six library databases were examined from the time they were developed to February 2019. Studies were included if they involved testing of an activity aimed at reducing medication errors in adult medical and surgical settings in hospital. Statistical analysis was used to look at the success of different types of activities.
Results: A total of 34 studies were included with 12 activity types identified. Statistical analysis showed that prescribing errors were reduced by pharmacists matching medications, computers matching medications, partnerships with pharmacists, prescriber education, medication matching by trained physicians, and computerised physician order entry (CPOE). Medication-giving errors were reduced by the use of CPOE and an automated medication distribution system. The combination of different activity types were also shown to be successful in reducing prescribing or medication-giving errors. No activities were found to be successful in reducing errors relating to supplying medications. Most studies were conducted at one hospital with reviewing patient charts being the most common way for collecting information about medication errors. In 21 out of 34 articles, researchers examined the effect of activity types on patient harm caused by medication errors. Many studies did not involve the use of a control group that does not receive the activity.
Conclusion: A number of activity types were shown to be successful in reducing prescribing and medication-giving errors. New directions for future research should examine activities comprising health professionals working together.
Keywords: hospitals; medical order entry systems; medication errors; medication reconciliation; medication therapy management; nurses; patient safety; pharmacists; physicians; systematic review.
© The Author(s), 2020.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Barker KN, Mikeal RL, Pearson RE, et al. Medication errors in nursing homes and small hospitals. Am J Hosp Pharm 1982; 39: 987–991. - PubMed
-
- Fahimi F, Abbasi Nazari M, Abrishami R, et al. Transcription errors observed in a teaching hospital. Arch Iran Med 2009; 12: 173–175. - PubMed
-
- Makary MA, Daniel M. Medical error—the third leading cause of death in the US. BMJ 2016; 353: i2139. - PubMed
-
- Donaldson LJ, Kelley ET, Dhingra-Kumar N, et al. Medication without harm: WHO’s third global patient safety challenge. Lancet 2017; 389: 1680–1681. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
