

Distinct clinicopathologic factors and prognosis based on the presence of ground-glass opacity components in patients with resected stage I non-small cell lung cancer
- PMID: 33240982
- PMCID: PMC7576059
- DOI: 10.21037/atm-20-4971
Distinct clinicopathologic factors and prognosis based on the presence of ground-glass opacity components in patients with resected stage I non-small cell lung cancer
Abstract
Background: This study was to investigate the prognostic value of ground-glass opacity(GGO) components and to evaluate distinct the clinicopathological variables of survival outcomes for the pure-GGO, part-solid and solid groups of patients with resected stage I non-small cell lung cancer (NSCLC).
Methods: We retrospectively reviewed the structured data for stage I NSCLC patients who had undergone the curative-intent surgical resection in the Lung Cancer Database of West China Hospital from 2009 to 2016. The eligible patients were divided into the pure-GGO, part-solid and solid groups according to the radiological manifestation. Univariate and multivariate Cox regression analyses were performed between the 3 groups. And we further evaluated the clinicopathological variables in each group separately.
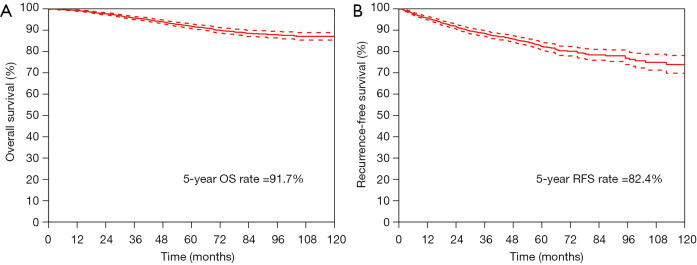
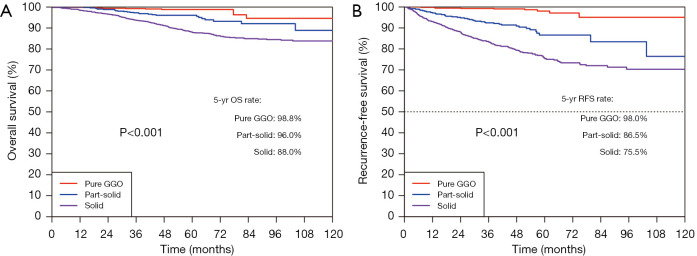
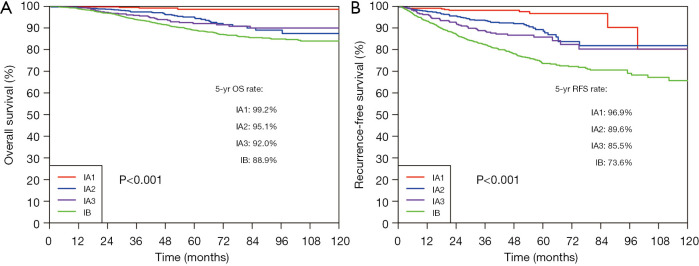
Results: Among a total of 2,775 eligible patients enrolled into the cohort were 1,587 (57.19%) in the solid group, 508 (18.31%) in the part-solid group, and 680 (24.50%) in the pure-GGO group. The 5-year overall survival (OS) and recurrence-free survival (RFS) rates were 98.8% and 98.0% in the pure-GGO group, 96.0% and 86.5% in the part-solid group, and 88.0% and 75.5% in the solid group, respectively (P<0.001). Presence of GGO components was a significantly favorable prognosticator (HR =0.415, 95% CI: 0.286-0.601). Different groups had distinct prognostic factors. LVI was the shared risk factor for groups with presence of GGO components in both part-solid and pure-GGO groups. Pathological stage (IA or IB) was influential exclusively for the pure-GGO group. In the solid group, females, younger patients, and patients without VPI had better survival. But such independent significance did not exist in the other two groups.
Conclusions: GGO component was a strong prognosticator of better prognosis in resected patients with stage I NSCLC. Prognostic factors and survival outcomes were disparate among the pure-GGO, part-solid, and solid group. Our results support the proposal that the next edition tumor-node-metastasis (TNM) classification should consider the importance of GGO components as a new T descriptor.
Keywords: Non-small cell lung cancer (NSCLC); ground-glass opacity (GGO); part-solid nodule; solid nodule; survival analysis.
2020 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/atm-20-4971). The authors have no conflicts of interest to declare.
Figures
References
-
- Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018;391:1023-75. 10.1016/S0140-6736(17)33326-3 - DOI - PMC - PubMed
-
- De Koning HJ, Van Der Aalst K, Ten Haaf M, et al. PL02.05 Effects of volume CT lung cancer screening: mortality results of the NELSON randomised-controlled population based trial. J Thorac Oncol 2018;13:S185. 10.1016/j.jtho.2018.08.012 - DOI
LinkOut - more resources
Full Text Sources