

Management of Atrial Fibrillation in Older Patients by Morbidity Burden: Insights From Get With The Guidelines-Atrial Fibrillation
- PMID: 33241750
- PMCID: PMC7763767
- DOI: 10.1161/JAHA.120.017024
Management of Atrial Fibrillation in Older Patients by Morbidity Burden: Insights From Get With The Guidelines-Atrial Fibrillation
Abstract
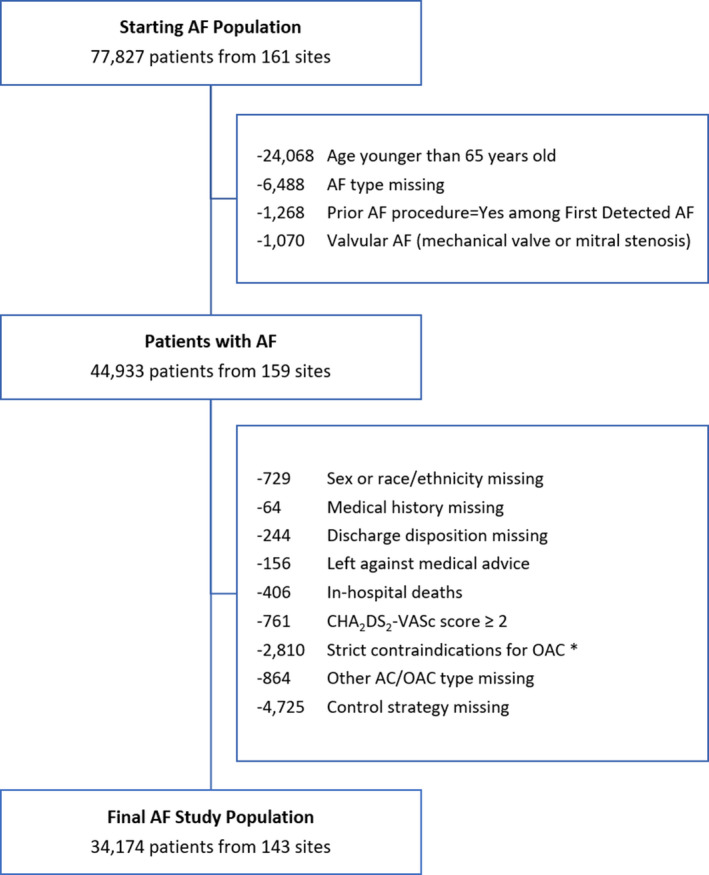
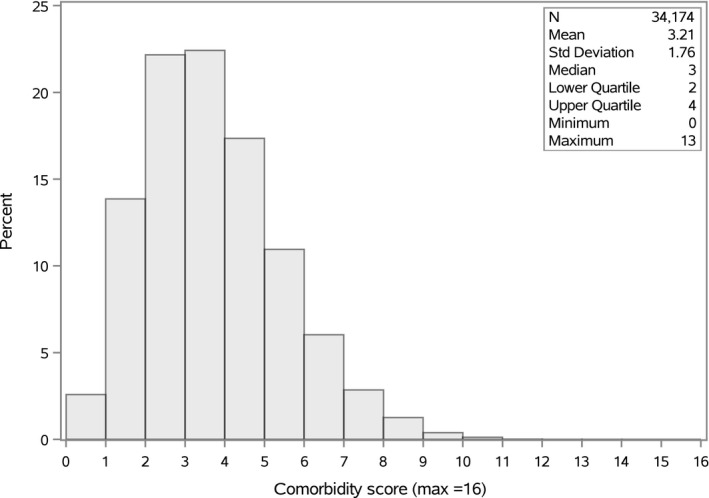
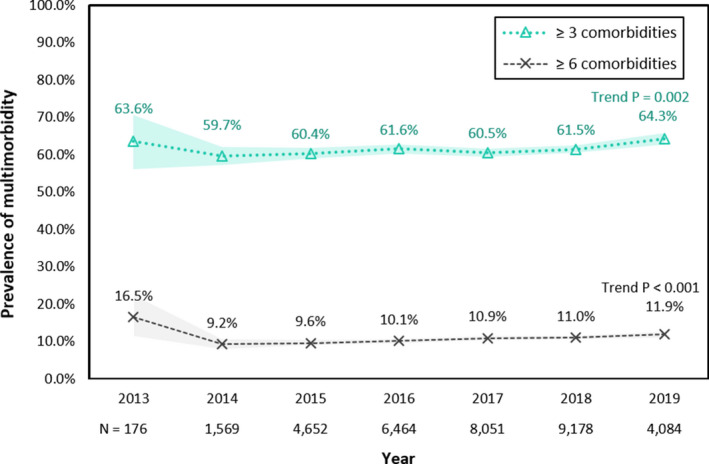
Background Knowledge is scarce regarding how multimorbidity is associated with therapeutic decisions regarding oral anticoagulants (OACs) in patients with atrial fibrillation. Methods and Results We conducted a cross-sectional study of hospitalized patients with atrial fibrillation using the Get With The Guidelines-Atrial Fibrillation registry from 2013 to 2019. We identified patients ≥65 years and eligible for OAC therapy. Using 16 available comorbidity categories, patients were stratified by morbidity burden. A multivariable logistic regression model was used to determine the odds of receiving OAC prescription at discharge by morbidity burden. We included 34 174 patients with a median (interquartile range) age of 76 (71-83) years, 56.6% women, and 41.9% were not anticoagulated at admission. Of these patients, 38.6% had 0 to 2 comorbidities, 50.7% had 3 to 5 comorbidities, and 10.7% had ≥6 comorbidities. The overall discharge OAC prescription was high (85.6%). The prevalence of patients with multimorbidity increased from 59.7% in 2014 to 64.3% in 2019 (P trend=0.002). Using 0 to 2 comorbidities as the reference, the adjusted odds ratio (95% CI) of OAC prescription were 0.93 (0.82, 1.05) for patients with 3 to 5 comorbidities and 0.72 (0.60, 0.86) for patients with ≥6 comorbidities. In those with ≥6 comorbidities, the most common reason for nonprescription of OACs were frequent falls/frailty (31.0%). Conclusions In a contemporary quality-of-care database of hospitalized patients with atrial fibrillation eligible for OAC therapy, multimorbidity was common. A higher morbidity burden was associated with a lower odds of OAC prescription. This highlights the need for interventions to improve adherence to guideline-recommended anticoagulation in multimorbid patients with atrial fibrillation.
Keywords: anticoagulation; atrial fibrillation; comorbidities; multimorbidity; oral anticoagulants; prescription; quality of care.
Conflict of interest statement
Gregg C. Fonarow is a consultant for Abbott, Amgen, AstraZeneca, Bayer, CHF Solutions, Merck, Medtronic, and Novartis. Angela Lowenstern is funded through NIH T‐32 training grant #5 T32 HL069749‐14. John H. Alexander has received research support from Boehringer Ingelheim, Bristol‐Myers Squibb, CryoLife, CSL Behring, Glaxosmithkline, US Food and Drug Administration, US National Institutes of Health, and XaTek and consulting/honoraria from AbbVie, Bayer, Bristol‐Myers Squibb, CryoLife, CSL Behring, Novo Nordisk, Pfizer, Portola, Quantum Genomics, US Department of Veterans Affairs, XaTek, Zafgen. Anne B. Curtis is on the advisory board of Janssen Pharmaceuticals; Abbott, Sanofi Aventis, Milestone Pharmaceuticals; honoraria for speaking: Abbott, Medtronic, Inc.; data monitoring board: Medtronic, Inc. Renato D. Lopes reported grants and personal fees from Bristol‐Myers Squibb and Pfizer, personal fees from Boehringer Ingelheim and Bayer AG and grants from Amgen Inc, GlaxoSmithKline, Medtronic PLC, and Sanofi Aventis outside the submitted work. Sana Al‐Khatib receives consulting fees from Milestone Pharmaceuticals, consulting and speaking fees from Medtronic, speaking fees from BMS/Pfizer, and research and speaking fees from Abbott. The remaining authors have no disclosures to report.
Figures
References
-
- Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, Meinow B, Fratiglioni L. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10:430–439. - PubMed
