

A novel haemocytometric COVID-19 prognostic score developed and validated in an observational multicentre European hospital-based study
- PMID: 33241996
- PMCID: PMC7732342
- DOI: 10.7554/eLife.63195
A novel haemocytometric COVID-19 prognostic score developed and validated in an observational multicentre European hospital-based study
Abstract
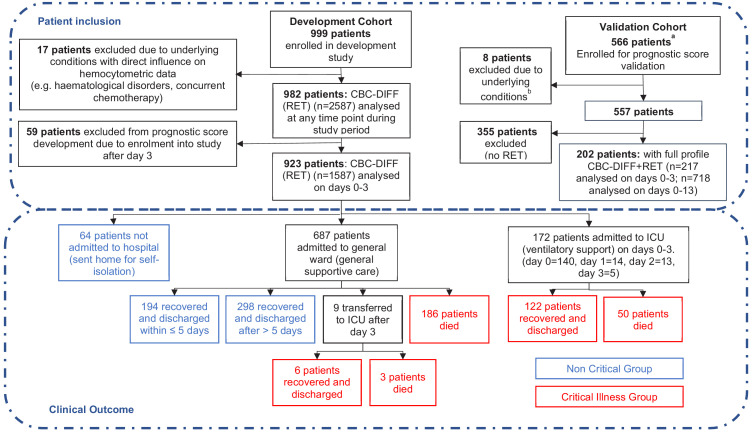
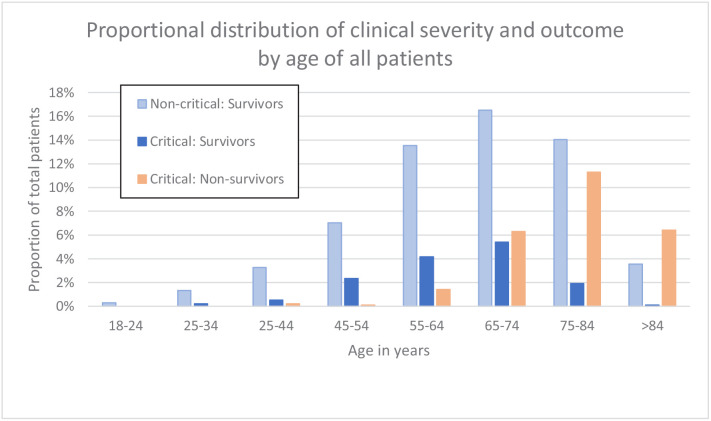
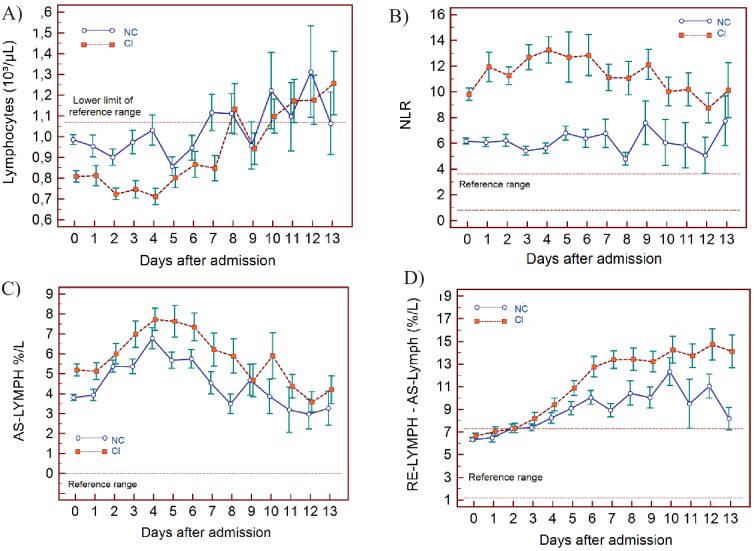
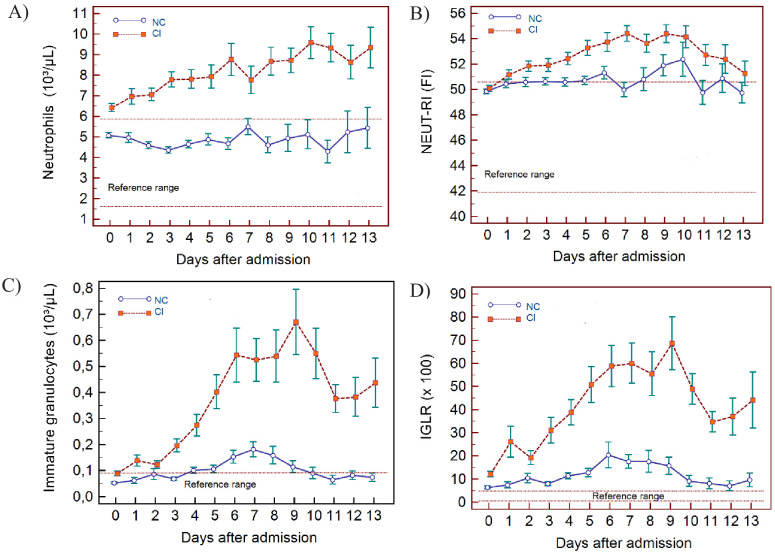
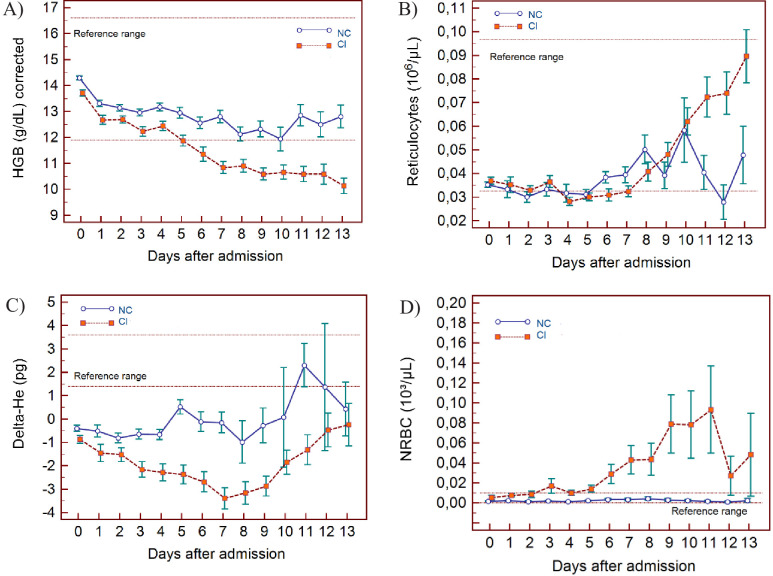
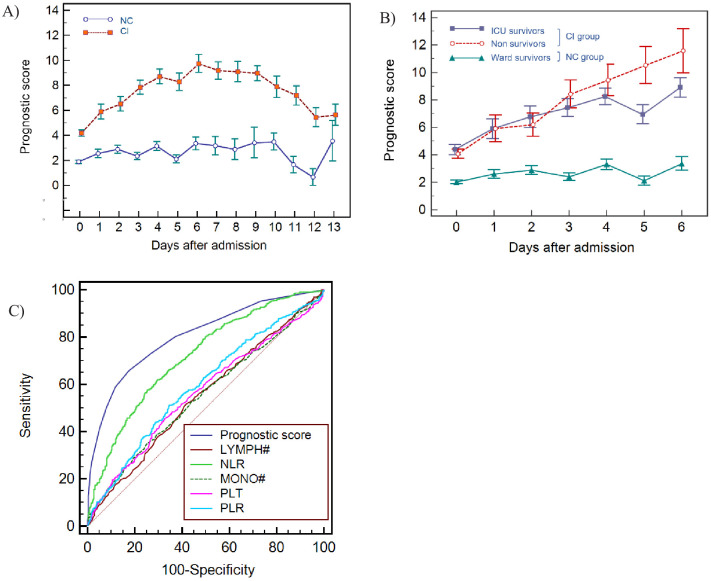
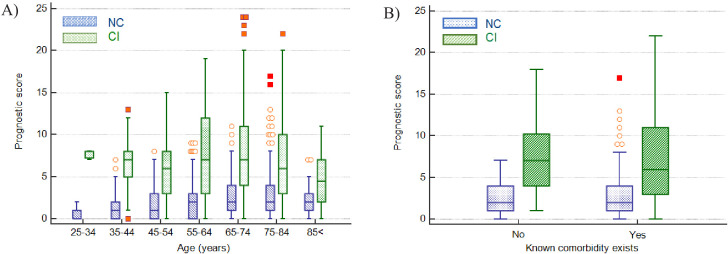
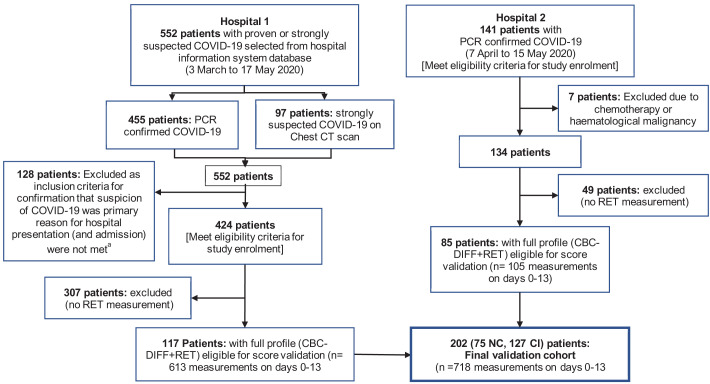
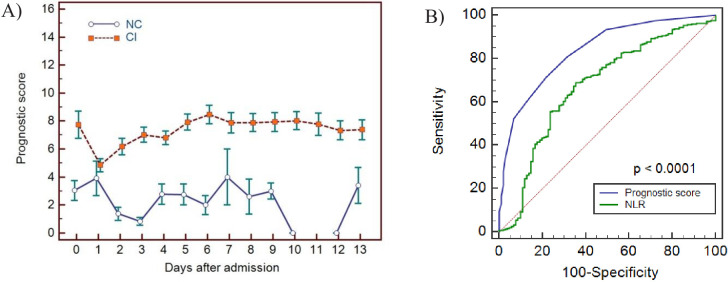
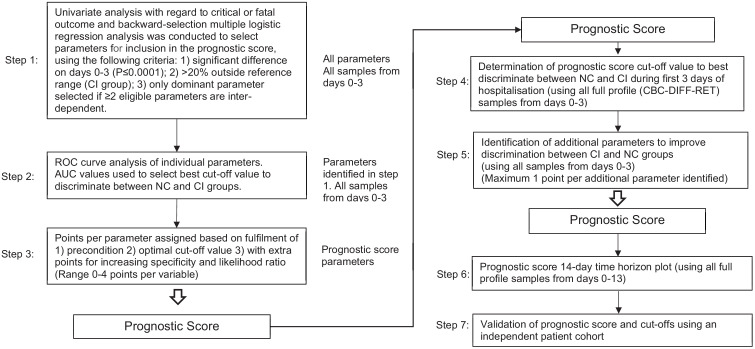
COVID-19 induces haemocytometric changes. Complete blood count changes, including new cell activation parameters, from 982 confirmed COVID-19 adult patients from 11 European hospitals were retrospectively analysed for distinctive patterns based on age, gender, clinical severity, symptom duration, and hospital days. The observed haemocytometric patterns formed the basis to develop a multi-haemocytometric-parameter prognostic score to predict, during the first three days after presentation, which patients will recover without ventilation or deteriorate within a two-week timeframe, needing intensive care or with fatal outcome. The prognostic score, with ROC curve AUC at baseline of 0.753 (95% CI 0.723-0.781) increasing to 0.875 (95% CI 0.806-0.926) on day 3, was superior to any individual parameter at distinguishing between clinical severity. Findings were confirmed in a validation cohort. Aim is that the score and haemocytometry results are simultaneously provided by analyser software, enabling wide applicability of the score as haemocytometry is commonly requested in COVID-19 patients.
Keywords: COVID-19; complete blood count; haemocytometry; human; intensive care; medicine; prognostic score.
© 2020, Linssen et al.
Conflict of interest statement
JL, JS, MM is a permanent employee of Sysmex Europe GMBH who provided free of charge study reagents to the study centres. AE, MB, MS, GP, Sv, HR, AV, JG, JR, Ed, IM, AD, VS, HA, KD, SB, LV, YK, ML No competing interests declared, Av has an ad hoc consultancy agreement with Sysmex Europe GMBH who provided free of charge study reagents to the study centres.
Figures


References
-
- Caramelo F, Ferreira N, Oliveiros B. Estimation of risk factors for COVID-19 mortality - preliminary results. medRxiv. 2020 doi: 10.1101/2020.02.24.20027268. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
