

Safety and efficacy of amantadine, modafinil, and methylphenidate for fatigue in multiple sclerosis: a randomised, placebo-controlled, crossover, double-blind trial
- PMID: 33242419
- PMCID: PMC7772747
- DOI: 10.1016/S1474-4422(20)30354-9
Safety and efficacy of amantadine, modafinil, and methylphenidate for fatigue in multiple sclerosis: a randomised, placebo-controlled, crossover, double-blind trial
Abstract
Background: Methylphenidate, modafinil, and amantadine are commonly prescribed medications for alleviating fatigue in multiple sclerosis; however, the evidence supporting their efficacy is sparse and conflicting. Our goal was to compare the efficacy of these three medications with each other and placebo in patients with multiple sclerosis fatigue.
Methods: In this randomised, placebo-controlled, four-sequence, four-period, crossover, double-blind trial, patients with multiple sclerosis who reported fatigue and had a Modified Fatigue Impact Scale (MFIS) score of more than 33 were recruited at two academic multiple sclerosis centres in the USA. Participants received oral amantadine (up to 100 mg twice daily), modafinil (up to 100 mg twice daily), methylphenidate (up to 10 mg twice daily), or placebo, each given for up to 6 weeks. All patients were intended to receive all four study medications, in turn, in one of four different sequences with 2-week washout periods between medications. A biostatistician prepared a concealed allocation schedule, stratified by site, randomly assigning a sequence of medications in approximately a 1:1:1:1 ratio, in blocks of eight, to a consecutive series of numbers. The statistician and pharmacists had no role in assessing the participants or collecting data, and the participants, caregivers, and assessors were masked to allocation. The primary outcome measure was the MFIS measured while taking the highest tolerated dose at week 5 of each medication period, analysed by use of a linear mixed-effect regression model. This trial is registered with ClinicalTrials.gov, NCT03185065 and is closed.
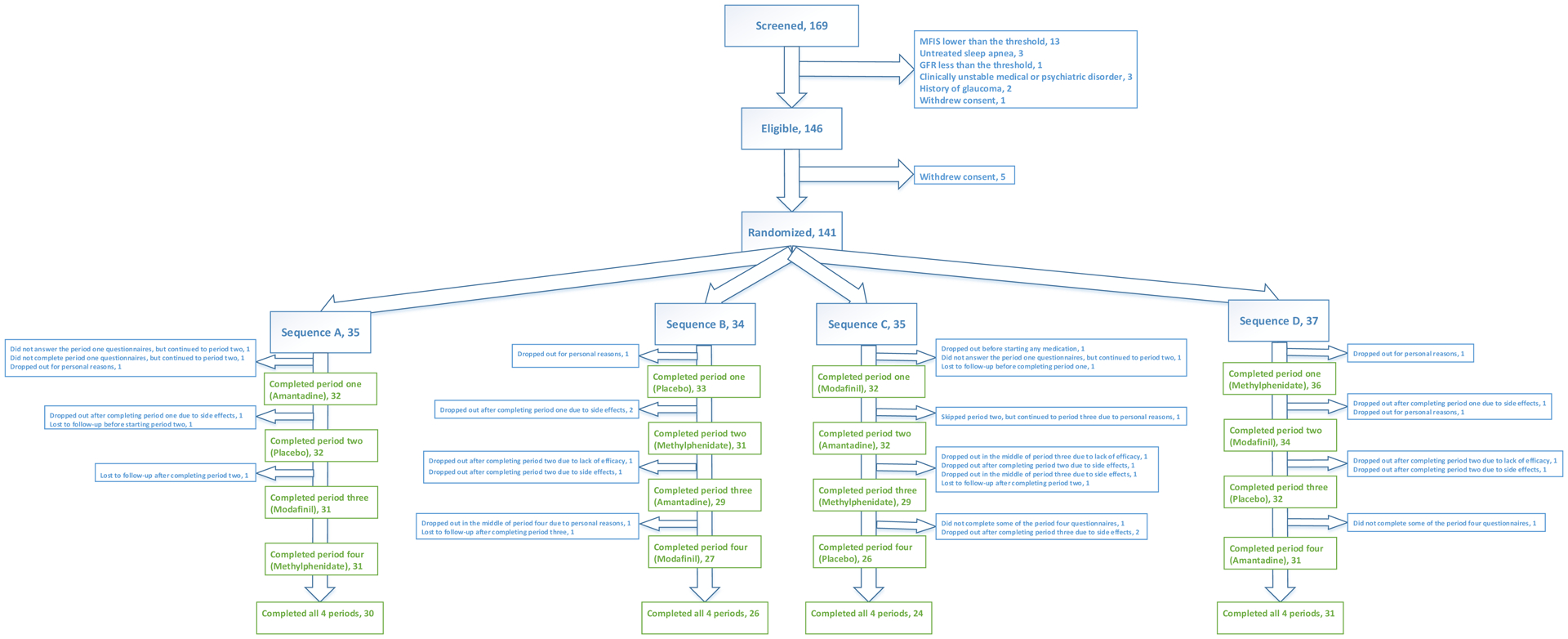
Findings: Between Oct 4, 2017, and Feb 27, 2019, of 169 patients screened, 141 patients were enrolled and randomly assigned to one of four medication administration sequences: 35 (25%) patients to the amantadine, placebo, modafinil, and methylphenidate sequence; 34 (24%) patients to the placebo, methylphenidate, amantadine, and modafinil sequence; 35 (25%) patients to the modafinil, amantadine, methylphenidate, and placebo sequence; and 37 (26%) patients to the methylphenidate, modafinil, placebo, and amantadine sequence. Data from 136 participants were available for the intention-to-treat analysis of the primary outcome. The estimated mean values of MFIS total scores at baseline and the maximal tolerated dose were as follows: 51·3 (95% CI 49·0-53·6) at baseline, 40·6 (38·2-43·1) with placebo, 41·3 (38·8-43·7) with amantadine, 39·0 (36·6-41·4) with modafinil, and 38·6 (36·2-41·0) with methylphenidate (p=0·20 for the overall medication effect in the linear mixed-effect regression model). As compared with placebo (38 [31%] of 124 patients), higher proportions of participants reported adverse events while taking amantadine (49 [39%] of 127 patients), modafinil (50 [40%] of 125 patients), and methylphenidate (51 [40%] of 129 patients). Three serious adverse events occurred during the study (pulmonary embolism and myocarditis while taking amantadine, and a multiple sclerosis exacerbation requiring hospital admission while taking modafinil).
Interpretation: Amantadine, modafinil, and methylphenidate were not superior to placebo in improving multiple sclerosis fatigue and caused more frequent adverse events. The results of this study do not support an indiscriminate use of amantadine, modafinil, or methylphenidate for the treatment of fatigue in multiple sclerosis.
Funding: Patient-Centered Outcomes Research Institute.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests
BN has received funding from the National MS Society (NMSS), PCORI, and Genentech and personal fees from Jazz Pharmaceutical. CM has received funding from PCORI. EW has received personal fee from Jazz Pharmaceutical, Emerald, and DBV. KK has received funding from PCORI, NMSS and Biogen. EM has received research support from Teva, grants from Sun Pharma, Sanofi Genzyme, Biogen, and personal fees from UpToDate. NR, BM, CC, JC, MM, AR, CA, SA, CJ declare no competing interests.
Figures
Comment in
-
Are drugs for multiple sclerosis fatigue just placebos?Lancet Neurol. 2021 Jan;20(1):20-21. doi: 10.1016/S1474-4422(20)30415-4. Epub 2020 Nov 23. Lancet Neurol. 2021. PMID: 33242420 No abstract available.
References
-
- Krupp L Fatigue is intrinsic to multiple sclerosis (MS) and is the most commonly reported symptom of the disease. Mult Scler 2006; 12: 367–8. - PubMed
-
- Lerdal A, Celius EG, Krupp L, Dahl AA. A prospective study of patterns of fatigue in multiple sclerosis. Eur J Neurol 2007; 14: 1338–43. - PubMed
-
- Zifko UA. Management of Fatigue in Patients with Multiple Sclerosis. Drugs 2004; 64: 1295–304. - PubMed
-
- Penner I-K, Paul F. Fatigue as a symptom or comorbidity of neurological diseases. Nat Rev Neurol 2017; 13: 662–75. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
