

Sex Disparities in COVID-19 Severity and Outcome: Are Men Weaker or Women Stronger?
- PMID: 33242856
- PMCID: PMC7900484
- DOI: 10.1159/000513346
Sex Disparities in COVID-19 Severity and Outcome: Are Men Weaker or Women Stronger?
Abstract
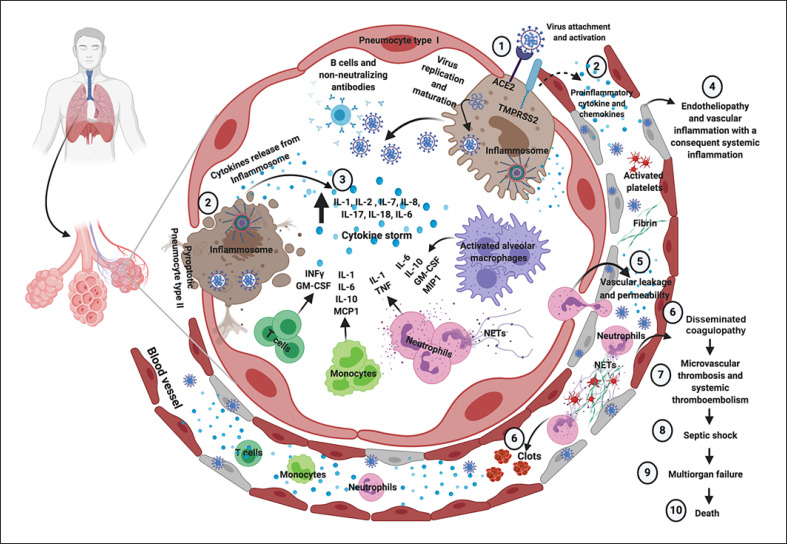
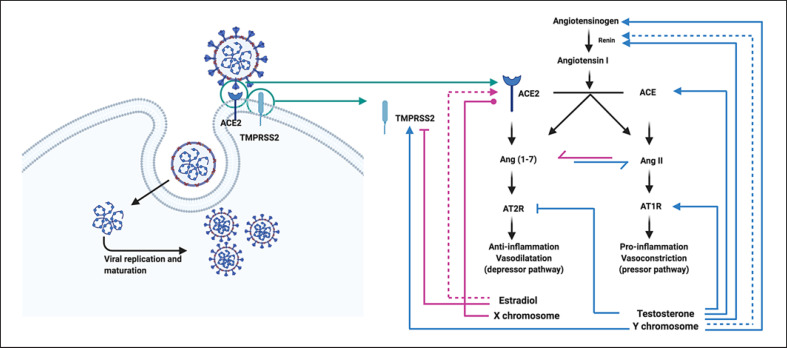
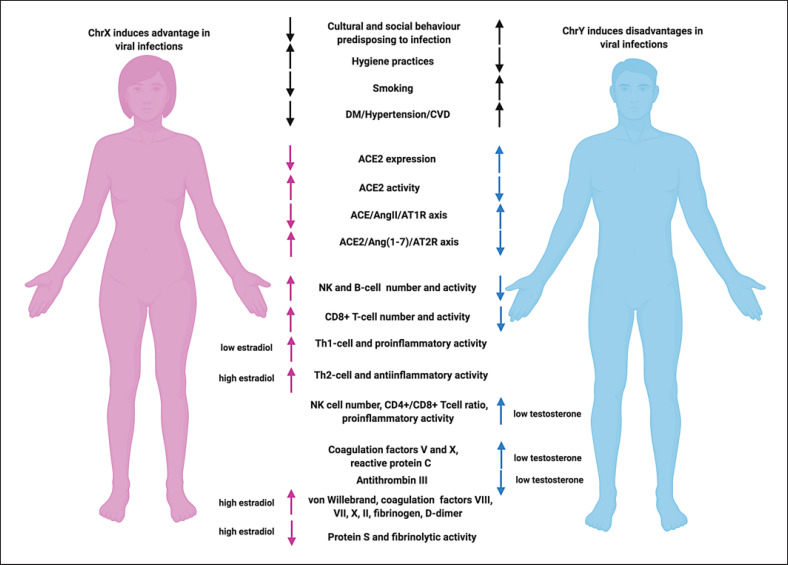
The coronavirus disease 2019 (COVID-19) outbreak, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a global public health issue which has profound effects on most aspects of societal well-being, including physical and mental health. A plethora of studies globally have suggested the existence of a sex disparity in the severity and outcome of COVID-19 patients, mainly due to mechanisms of virus infection, immune response to the virus, development of systemic inflammation, and consequent systemic complications, particularly thromboembolism. Epidemiological data report a sex difference in the severity of COVID-19, with a more favorable course of the disease in women compared to men regardless of age, although the rate of SARS-CoV-2 infection seems to be similar in both sexes. Sex hormones, including androgens and estrogens, may not only impact virus entry and load, but also shape the clinical manifestations, complications, and ultimately the outcome of the disease. The current review comprehensively summarizes the current literature on sex disparities in susceptibility and outcome of COVID-19 as well as the literature underpinning the pathophysiological and molecular mechanisms, which may provide a rationale to a sex disparity. These mechanisms include sex hormone influence on factors that facilitate virus entry and priming, immune and inflammatory response, as well as coagulation and thrombosis diathesis. Based on present evidence, women appear to be relatively protected from COVID-19 because of a more effective immune response and a less pronounced systemic inflammation, with consequent moderate clinical manifestations of the disease, together with a lesser predisposition to thromboembolism. Conversely, men appear to be particularly susceptible to COVID-19 because of a less effective immune response with consequent severe clinical manifestations of the disease, together with a greater predisposition to thromboembolism. In the elderly, generally characterized by the phenomenon of inflammaging, sex disparities in overall mortality following SARS-CoV-2 infection are even more palpable as elderly men appear to be more prone to severe COVID-19 because of a greater predisposition to infections, a weaker immune defense, and an enhanced thrombotic state compared to women. The information revealed from the review highlights potential novel therapeutic approaches employing the administration of hormonal or antihormonal therapy in combination with antiviral drugs in COVID-19 patients.
Keywords: Androgens; COVID-19; Estrogens; Inflammaging; Sex disparity; Sex hormones.
© 2020 S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA. 2020 Aug;324((8)):782–93. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
