

Quxie Capsule Modulating Gut Microbiome and Its Association With T cell Regulation in Patients With Metastatic Colorectal Cancer: Result From a Randomized Controlled Clinical Trial
- PMID: 33243018
- PMCID: PMC7876934
- DOI: 10.1177/1534735420969820
Quxie Capsule Modulating Gut Microbiome and Its Association With T cell Regulation in Patients With Metastatic Colorectal Cancer: Result From a Randomized Controlled Clinical Trial
Abstract
Aim: Quxie capsule(QX), a TCM compound, had shown benefit on survival outcomes for metastatic colorectal cancer(mCRC) patients and could inhibit tumor growth through immune regulation. This study aimed to evaluate whether such effect is associated with gut microbiome modulation.
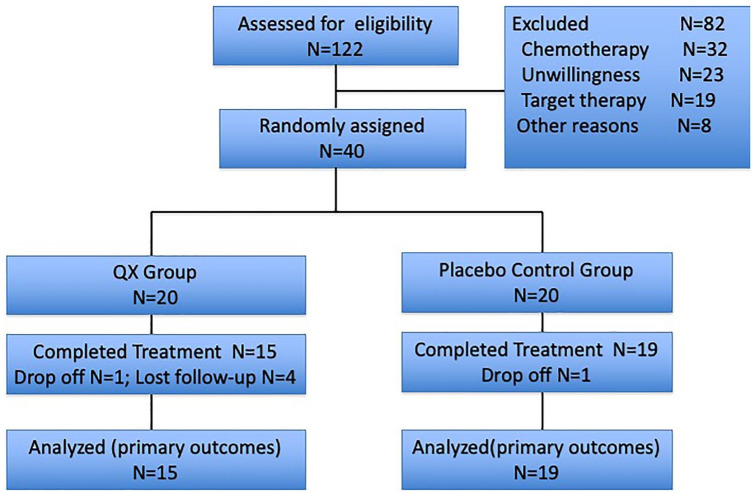
Method: We conducted a randomized double-blinded placebo controlled clinical trial in Xiyuan Hospital, China Academy of Chinese Medical Sciences. All patients were randomly assigned into QX or placebo control group. Before and after 1-month interventions, we collected patients' stool samples for microbiome analysis by 16s rRNA sequencing approaches, as well as blood samples to analyze T lymphocyte subsets by flow cytometry methods. Microbiome analysis among groups was done through bioinformation analysis platform. The study had been proved by the ethics committee of Xiyuan Hospital (2016XLA122-1) had been registered on Chinese Clinical Trial Registry (registration number: ChiCTR2000029599). All patients consented before enrollment.
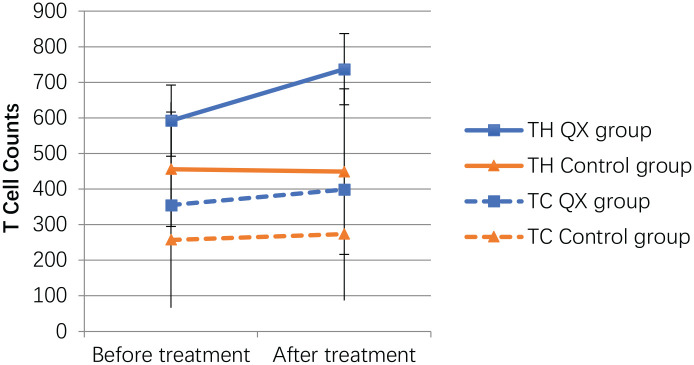
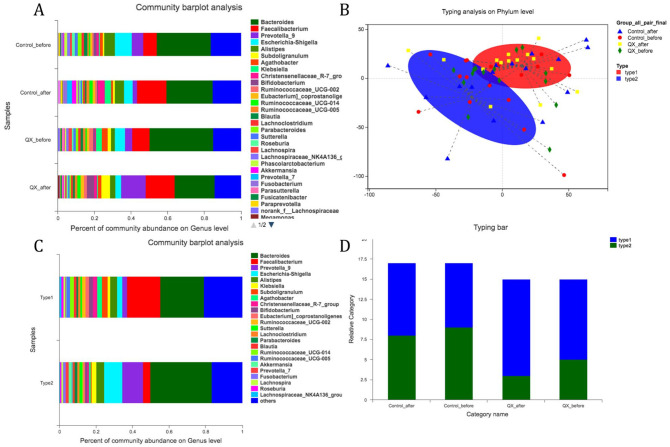
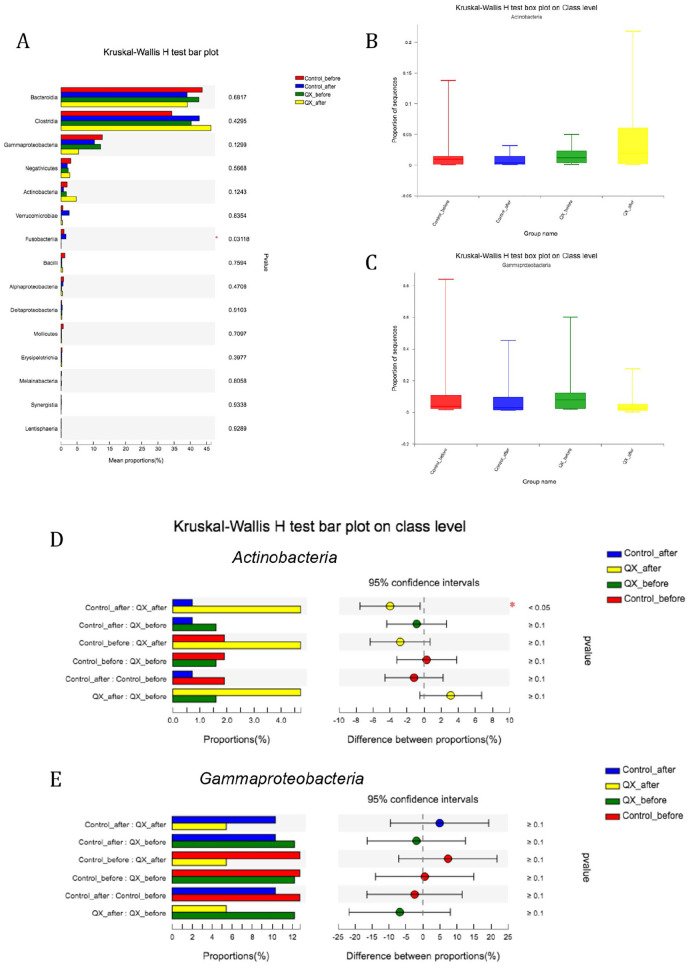
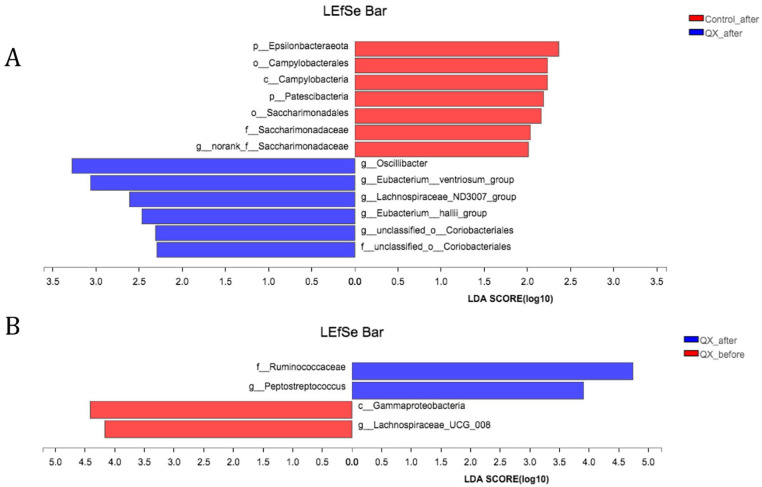
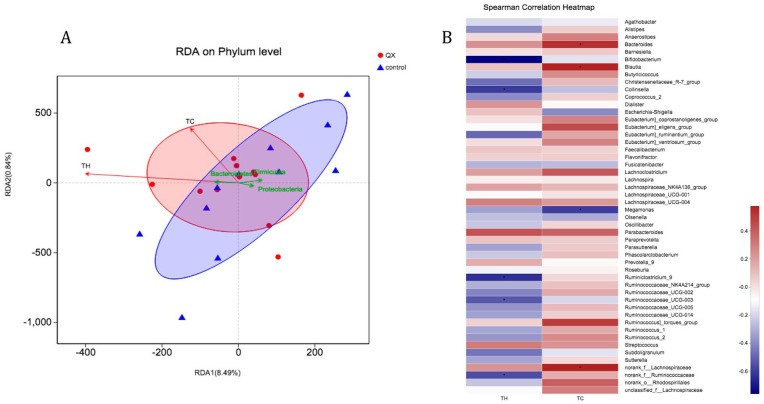
Results: We randomly assigned 40 patients and 34 were finally analyzed. Among them, 29% were female, with an average age of 63 years old, and 74% had liver or lung metastasis. Both CD4 T(TH) cell and CD8 T(TC) cell counts increased after QX treatment, while TH cells were significantly more in QX than in control group (737 vs 449, P = .024). Microbiome community analysis on Class level showed that the proportion of Actinobacteria declined in the control group, but significantly increased after QX treatments (0.83% vs 4.7%, P = .017). LEfSe analysis showed that after treatments, samples from QX group were highly related with Oscillibacter, Eubacterium, and Lachnospiraceae. RDA analysis showed that after QX interventions, stool samples and microbiome species had relevance with TC/TH cells counts but were not statistically significant. Heatmap analysis on Genus level revealed that after QX treatments, higher amounts of TH cells were significantly associated with less abundance of g_Bifidobacterium (coef. -0.76, P = .002), Collinsella (coef.-0.61, P = .02), Ruminiclostridium_9 (coef. -0.64, P = .01).
Conclusion: QX capsule could enhance TH cells level among mCRC patients and increase the abundance of gut anticancer bacteria such as Actinobacteria as well as butyrate-producing bacteria such as Lachnospiraceae. These results indicated that QX capsule might have the property of dual effects of antitumor and immunity enhancement, both mediated by the microbiome.
Keywords: T cell immunity; Traditional Chinese Medicine; gut microbiome; metastatic colorectal cancer; randomized clinical trial.
Conflict of interest statement
Figures
Similar articles
-
Conventional Therapy Combined With Quxie Capsule Modulating Gut Microbiome in Metastatic Colorectal Cancer Patients With the Third or Above Line Setting: Result From an Investigator-Initiated, Open-Label, Single-Arm, Phase II Study.Integr Cancer Ther. 2024 Jan-Dec;23:15347354241280390. doi: 10.1177/15347354241280390. Integr Cancer Ther. 2024. PMID: 39313964 Free PMC article. Clinical Trial.
-
Quxie Capsule Alleviates Colitis-associated Colorectal Cancer Through Modulating the Gut Microbiota and Suppressing A. fumigatus-induced Aerobic Glycolysis.Integr Cancer Ther. 2022 Jan-Dec;21:15347354221138534. doi: 10.1177/15347354221138534. Integr Cancer Ther. 2022. PMID: 36412281 Free PMC article.
-
Quxie Capsule Inhibits Colon Tumor Growth Partially Through Foxo1-Mediated Apoptosis and Immune Modulation.Integr Cancer Ther. 2019 Jan-Dec;18:1534735419846377. doi: 10.1177/1534735419846377. Integr Cancer Ther. 2019. PMID: 31030593 Free PMC article.
-
Effect of traditional Chinese medicine on gut microbiota in adults with type 2 diabetes: A systematic review and meta-analysis.Phytomedicine. 2021 Jul 15;88:153455. doi: 10.1016/j.phymed.2020.153455. Epub 2020 Dec 30. Phytomedicine. 2021. PMID: 33478831
-
Effect of Quxie capsule in patients with colorectal cancer: A systematic review and meta-analysis.Medicine (Baltimore). 2021 Feb 19;100(7):e24322. doi: 10.1097/MD.0000000000024322. Medicine (Baltimore). 2021. PMID: 33607767 Free PMC article.
Cited by
-
Interaction between microbiota and immunity and its implication in colorectal cancer.Front Immunol. 2022 Jul 29;13:963819. doi: 10.3389/fimmu.2022.963819. eCollection 2022. Front Immunol. 2022. PMID: 35967333 Free PMC article. Review.
-
Antitumour mechanisms of traditional Chinese medicine elicited by regulating tumour-associated macrophages in solid tumour microenvironments.Heliyon. 2024 Mar 2;10(5):e27220. doi: 10.1016/j.heliyon.2024.e27220. eCollection 2024 Mar 15. Heliyon. 2024. PMID: 38463777 Free PMC article. Review.
-
Traditional Chinese Medicines as Effective Reversals of Epithelial-Mesenchymal Transition Induced-Metastasis of Colorectal Cancer: Molecular Targets and Mechanisms.Front Pharmacol. 2022 Mar 4;13:842295. doi: 10.3389/fphar.2022.842295. eCollection 2022. Front Pharmacol. 2022. PMID: 35308223 Free PMC article. Review.
-
Traditional Chinese medicine for colorectal cancer treatment: potential targets and mechanisms of action.Chin Med. 2023 Feb 13;18(1):14. doi: 10.1186/s13020-023-00719-7. Chin Med. 2023. PMID: 36782251 Free PMC article. Review.
-
Adverse events of different PD-1 inhibitors in lung cancer patients: a real-world study.Ann Transl Med. 2022 Feb;10(4):183. doi: 10.21037/atm-21-6899. Ann Transl Med. 2022. PMID: 35280395 Free PMC article.
References
-
- Gao B, Wang R, Peng Y, et al. Effects of a homogeneous polysaccharide from Sijunzi decoction on human intestinal microbes and short chain fatty acids in vitro. J Ethnopharmacol. 2018;224:465-473. - PubMed
-
- Fakih MG. Metastatic colorectal cancer: current state and future directions. J Clin Oncol. 2015;33:1809-1824. - PubMed
-
- Dekker E, Tanis PJ, Vleugels JLA, et al. Colorectal cancer. Lancet. 2019;394:1467-1480. - PubMed
-
- Abdel-Rahman O. A real-world, population-based study of the outcomes of patients with metastatic colorectal cancer to the peritoneum treated with or without cytoreductive surgery. Int J Colorectal Dis. 2020;35:719-725. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
