

Heads-up Surgery: Endoscopes and Exoscopes for Otology and Neurotology in the Era of the COVID-19 Pandemic
- PMID: 33243372
- PMCID: PMC7522672
- DOI: 10.1016/j.otc.2020.09.024
Heads-up Surgery: Endoscopes and Exoscopes for Otology and Neurotology in the Era of the COVID-19 Pandemic
Abstract
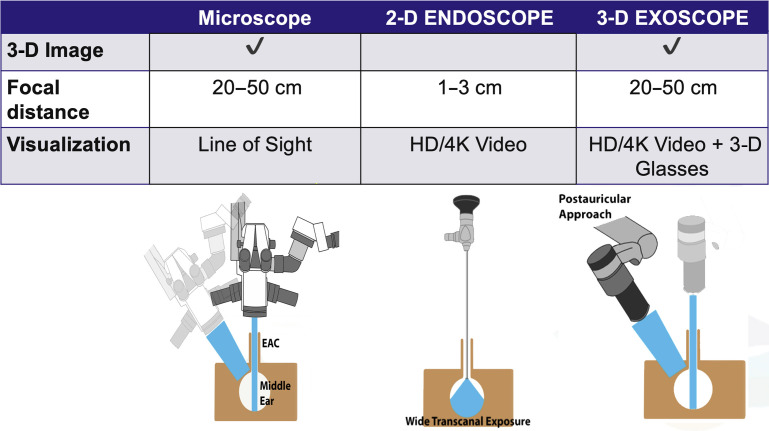
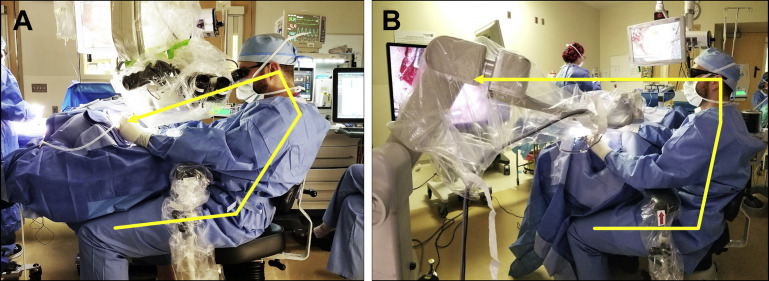
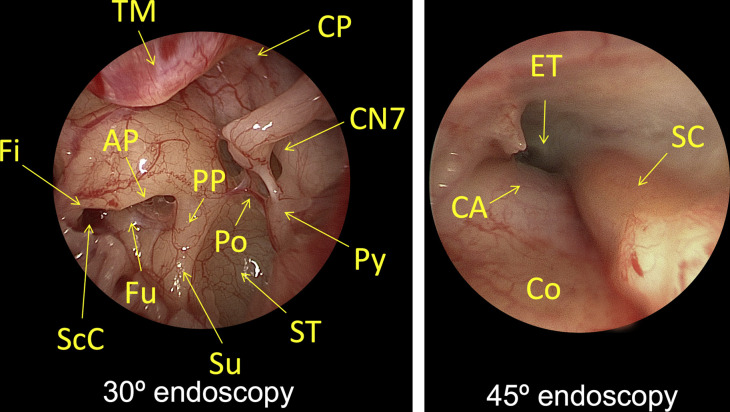
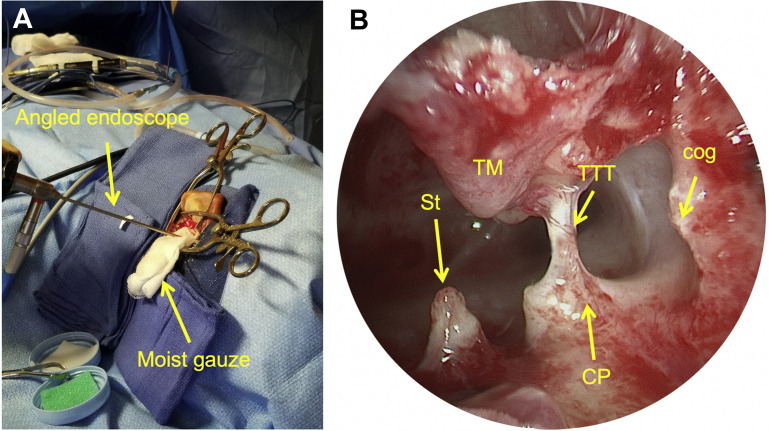
A new era of surgical visualization and magnification is poised to disrupt the field of otology and neurotology. The once revolutionary benefits of the binocular microscope now are shared with rigid endoscopes and exoscopes. These 2 modalities are complementary. The endoscope improves visualization of the hidden recesses through the external auditory canal or canal-up mastoidectomy. The exoscope provides an immersive visual experience and superior ergonomics compared with binocular microscopy. Endoscopes and exoscopes are poised to disrupt the standard of care for surgical visualization and magnification in otology and neurotology.
Keywords: Aerosol generating procedure; Endoscopic ear surgery; Ergonomics; Exoscopic ear surgery; Mastoidectomy; Microscope; Minimally-invasive; PPE.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Disclosure The senior author has financial relationships with 3NT Medical, Akouos, Frequency Therapeutics, Boston Pharmaceuticals, and Agilis.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
