

Cardiopulmonary Hemodynamics in Pulmonary Hypertension and Heart Failure: JACC Review Topic of the Week
- PMID: 33243385
- PMCID: PMC7703679
- DOI: 10.1016/j.jacc.2020.10.007
Cardiopulmonary Hemodynamics in Pulmonary Hypertension and Heart Failure: JACC Review Topic of the Week
Abstract
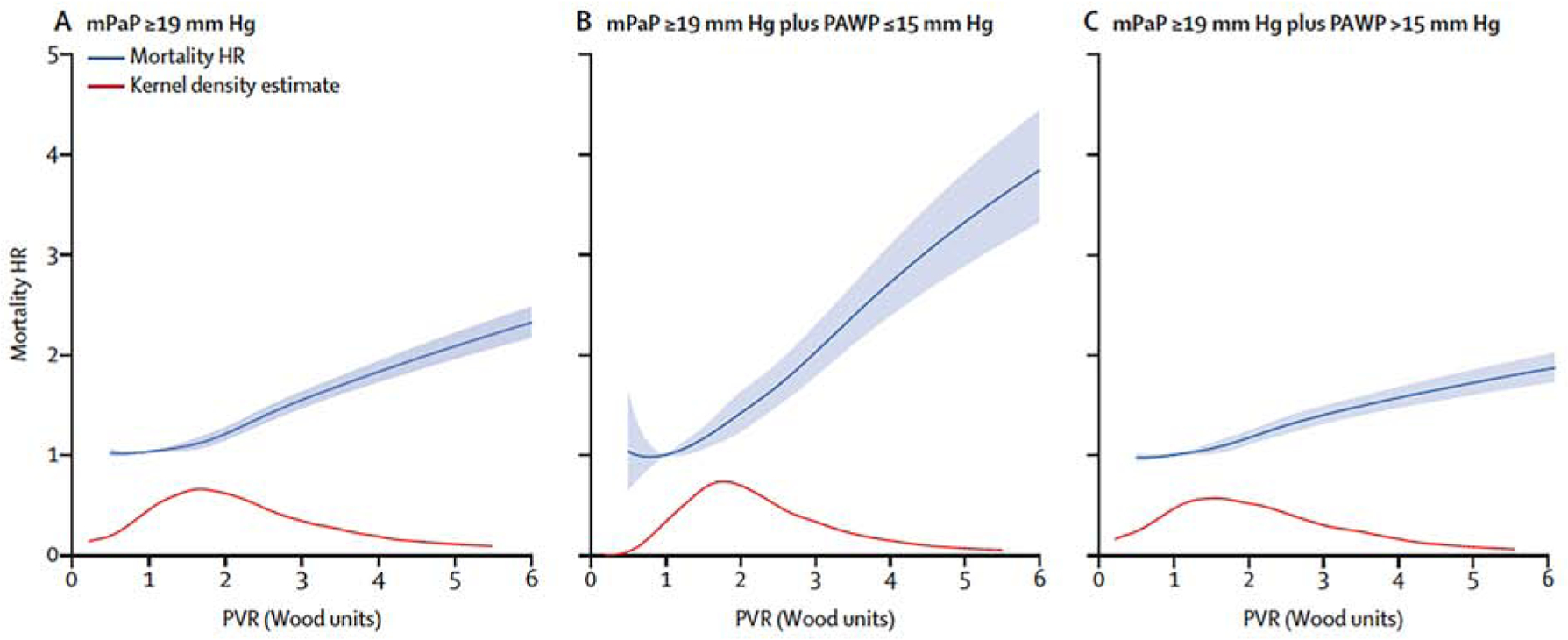
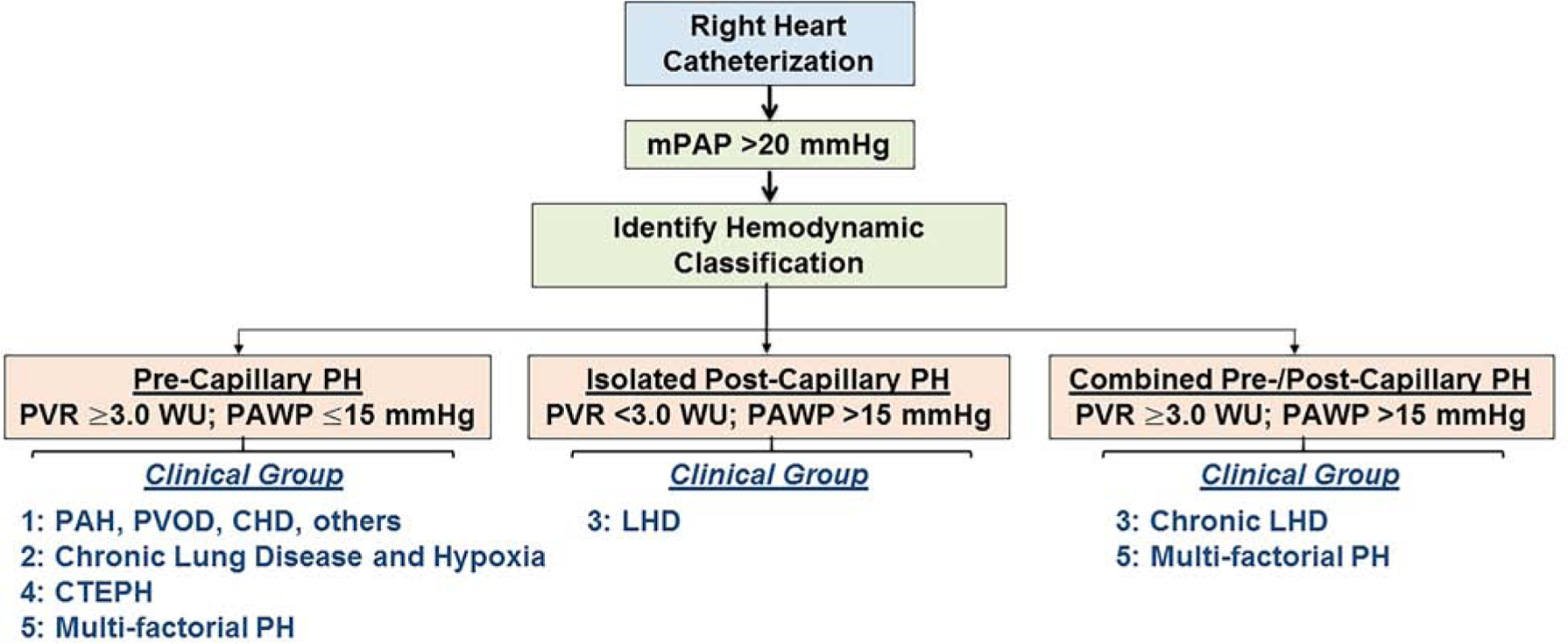
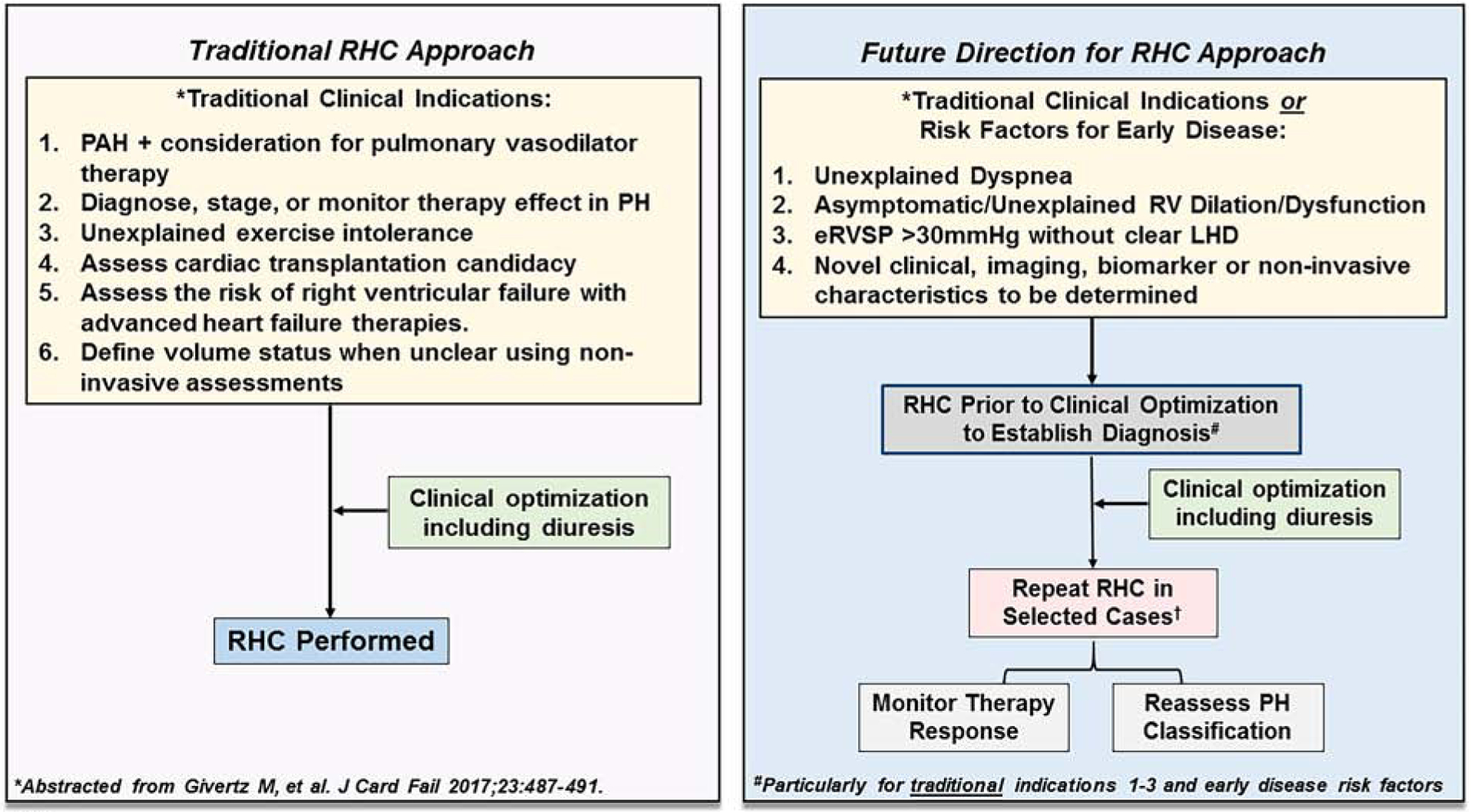
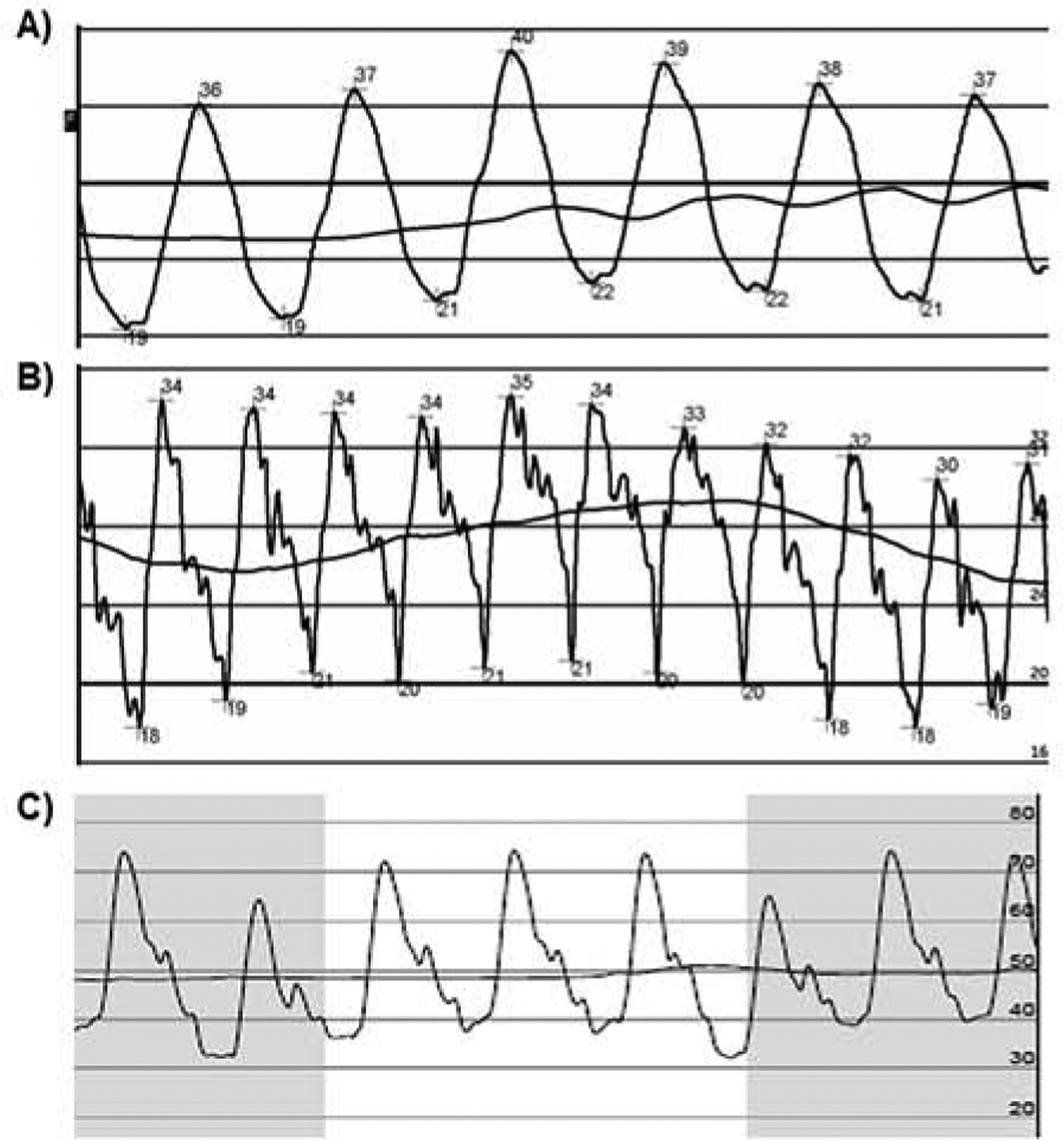
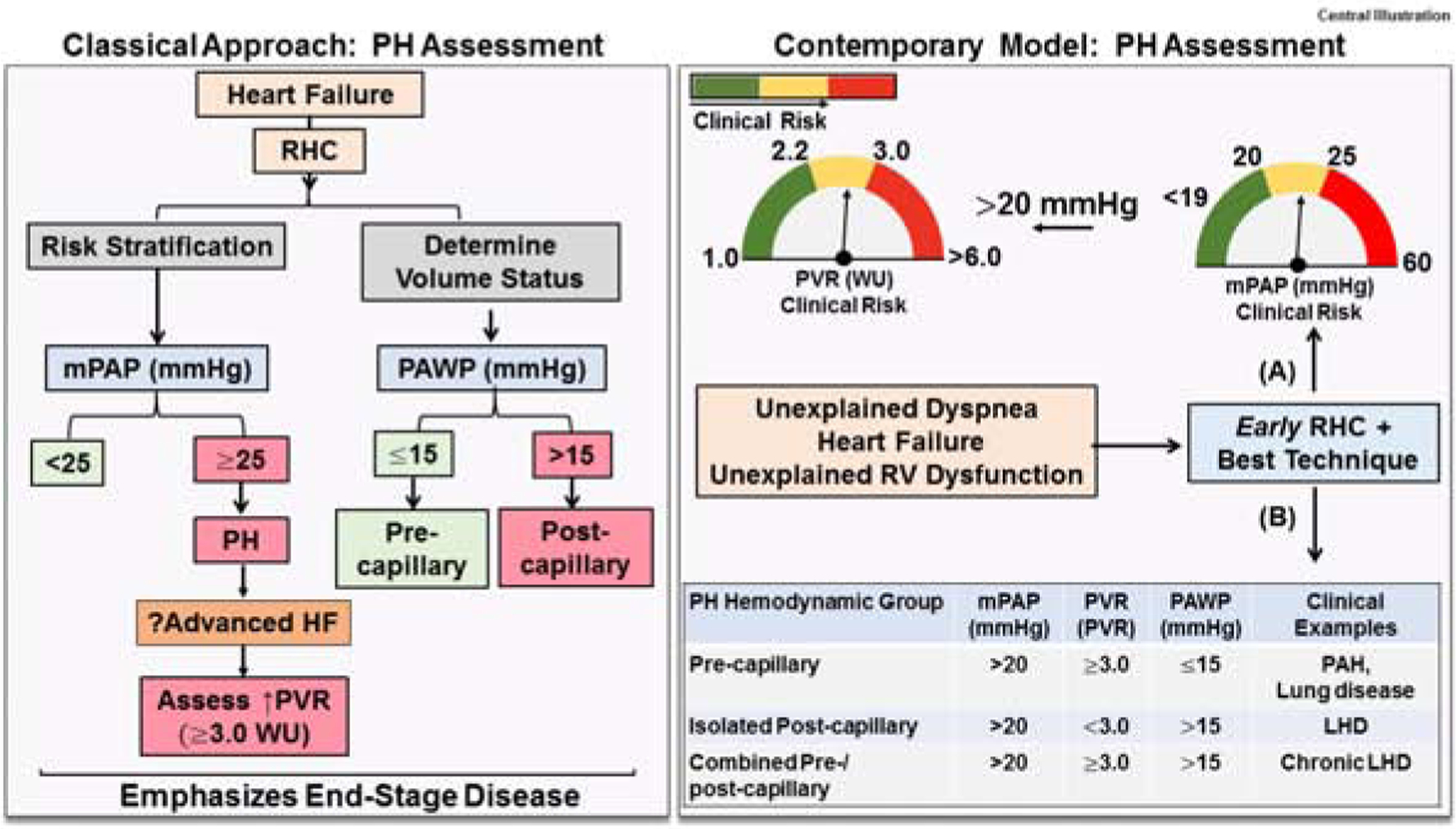
Pulmonary hypertension (PH) is an independent risk factor for adverse clinical outcome, particularly in left heart disease (LHD) patients. Recent advances have clarified the mean pulmonary artery pressure (mPAP) range that is above normal and is associated with clinical events, including mortality. This progress has for the first time resulted in a new clinical definition of PH that is evidenced-based, is inclusive of mPAP >20 mm Hg, and emphasizes early diagnosis. Additionally, pulmonary vascular resistance (PVR) 2.2 to 3.0 WU, considered previously to be normal, appears to associate with elevated clinical risk. A revised approach to classifying PH patients as pre-capillary, isolated post-capillary, or combined pre-/post-capillary PH now guides point-of-care diagnosis, risk stratification, and treatment. Exercise hemodynamic or confrontational fluid challenge studies may also aid decision-making for patients with PH-LHD or otherwise unexplained dyspnea. This collective progress in pulmonary vascular and heart failure medicine reinforces the critical importance of accurate hemodynamic assessment.
Keywords: heart failure; hemodynamics; pulmonary hypertension.
Published by Elsevier Inc.
Conflict of interest statement
Author Disclosures Dr. Maron is supported by grants R01HL139613-01, R01HL1535-02, U54HL119145, and R21HL145420, the Cardiovascular Medical Research Education Foundation, and McKenzie Family Charitable Trust, Boston Biomedical Innovations Center; has served as a consultant for Actelion; and is coinventor of patents or patent applications that are related to pulmonary hypertension (U.S. Patent #9,605,047; PCT/US2015/029672; Provisional ID: #62475955; Provisional ID: #24624; Provisional ID: #24622). Dr. Kovacs has received personal fees and nonfinancial support from Actelion, Bayer, GlaxoSmithKline, Merck Sharp and Dohme, Boehringer Ingelheim, Novartis, Chiesi, Vitalaire, Ferrer, and AOP outside the submitted work. Dr. Tedford has consulting relationships with Medtronic, Aria CV Inc., Arena Pharmaceuticals, and United Therapeutics; has served on a steering committee for Abbott, Acceleron, and Medtronic; has served on a research Advisory Board for Abiomed; and has performed hemodynamic core lab work for Actelion and Merck. Dr. Vaidya has served as a consultant for Bayer, United Therapeutics, Liquidia, and Actelion; and has served on the nonpromotional Speakers Bureau for Bayer, Actelion, and United Therapeutics. Dr. Bhatt has served on the Advisory Board of Cardax, CellProthera, Cereno Scientific, Elsevier Practice Update Cardiology, Level Ex, Medscape Cardiology, PhaseBio, PLx Pharma, and Regado Biosciences; has served on the Board of Directors of Boston VA Research Institute, Society of Cardiovascular Patient Care, and TobeSoft; has served as Chair of the American Heart Association Quality Oversight Committee, NCDR-ACTION Registry Steering Committee, and VA CART Research and Publications Committee; has served on data monitoring committees for Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute, for the PORTICO trial, funded by St. Jude Medical, now Abbott), Cleveland Clinic (including for the ExCEED trial, funded by Edwards), Contego Medical (Chair, PERFORMANCE 2), Canadian Medical and Surgical Knowledge Translation Research Group (clinical trial steering committees), Duke Clinical Research Institute, Mayo Clinic, Mount Sinai School of Medicine (for the ENVISAGE trial, funded by Daiichi-Sankyo), and Population Health Research Institute; has received honoraria from the American College of Cardiology (Senior Associate Editor, Clinical Trials and News, ACC.org; Vice-Chair, ACC Accreditation Committee), Baim Institute for Clinical Research (formerly Harvard Clinical Research Institute; RE-DUAL PCI clinical trial steering committee funded by Boehringer Ingelheim; AEGIS-II executive committee funded by CSL Behring), Belvoir Publications (Editor-in-Chief, Harvard Heart Letter), Duke Clinical Research Institute (clinical trial steering committees, including for the PRONOUNCE trial, funded by Ferring Pharmaceuticals), HMP Global (Editor-in-Chief, Journal of Invasive Cardiology), Journal of the American College of Cardiology (Guest Editor; Associate Editor), K2P (Co-Chair, interdisciplinary curriculum), Level Ex, Medtelligence/ReachMD (CME steering committees), MJH Life Sciences, Population Health Research Institute (for the COMPASS operations committee, publications committee, steering committee, and USA national co-leader, funded by Bayer), Slack Publications (Chief Medical Editor, Cardiology Today’s Intervention), Society of Cardiovascular Patient Care (Secretary/Treasurer), and WebMD (CME steering committees); has served as Deputy Editor of Clinical Cardiology; has received research funding from Abbott, Afimmune, Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Cardax, Chiesi, CSL Behring, Eisai, Ethicon, Ferring Pharmaceuticals, Forest Laboratories, Fractyl, Idorsia, Ironwood, Ischemix, Lexicon, Lilly, Medtronic, Pfizer, PhaseBio, PLx Pharma, Regeneron, Roche, Sanofi, Synaptic, and The Medicines Company; has received royalties from Elsevier (Editor, Cardiovascular Intervention: A Companion to Braunwald’s Heart Disease); has served as site co-investigator for Biotronik, Boston Scientific, CSI, St. Jude Medical (now Abbott), and Svelte; has served as a Trustee of the American College of Cardiology; and has performed unfunded research for FlowCo, Merck, Novo Nordisk, and Takeda. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Deaño RC, Glassner-Kolmin C, Rubenfire M, et al. Referral of patients with pulmonary hypertension diagnoses to tertiary pulmonary hypertension centers: the multicenter RePHerral study. JAMA Intern Med 2013;173:887–93. - PubMed
-
- Galie N, Barbera JA, Frost AE, et al. Initial use of ambrisentan plus tadalafil in pulmonary arterial hypertension. N Engl J Med 2015;373:834–44. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
